Japanese
English
- 有料閲覧
- Abstract 文献概要
- 1ページ目 Look Inside
I.はじめに
特異な筋病理所見を示すMyotubular myopathyは,1966年Spiroら24)による初めての報告では,筋細胞の発生過程での停止という機序が想定され,注目された。しかしその後,筋の変性所見を重視する報告3)や何らかの筋の再生過程の異常も一つの可能性として考えられることが提唱されている6)。本症の病因および単一疾患としての位置づけが確立されていない現在,なお新しい症例の集積と検討が望まれる。
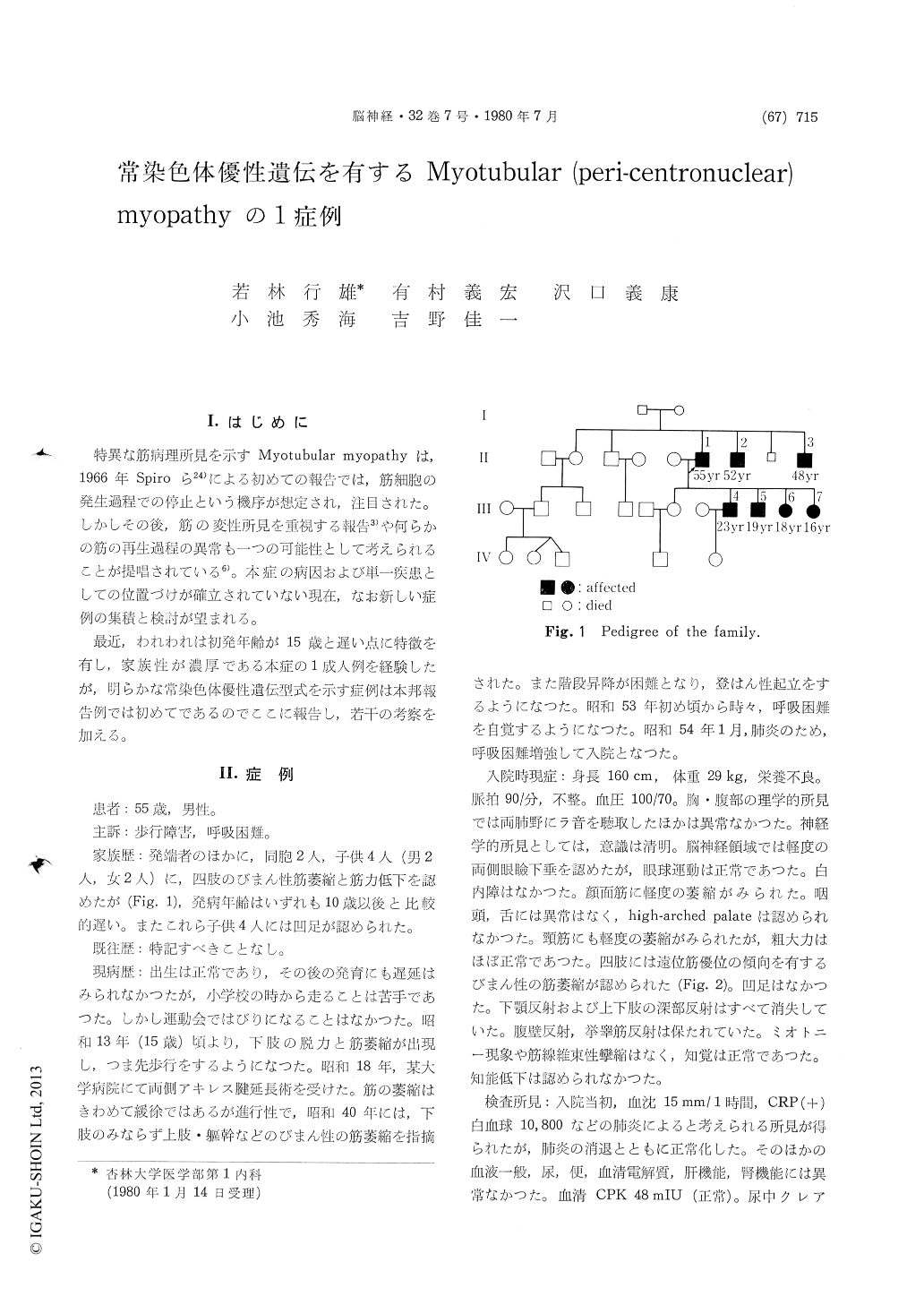
最近,われわれは初発年齢が15歳と遅い点に特徴を有し,家族性が濃厚である本症の1成人例を経験したが,明らかな常染色体優性遺伝型式を示す症例は本邦報告例では初めてであるのでここに報告し,若干の考察を加える。
A 55-year-old man, whose prenatal history, birth and infancy had been uneventful, developed nor-mally until the age of about 15 years, when weakness and muscle atrophy of the lower limbs appeared. At 20 years of age, he underwent an operation to lengthen Achilles tendons because of worsening pes equinus. The disease was slowly progressive, resulting in difficulty in going up and down stairs and rising from the floor, and at the age of 42, diffuse muscular atrophy was indicated by a physician not only in the lower limbs but also in the upper limbs and trunk. At the age of 54, one year before admission, he complained of some dyspnea. He was admitted to our hospital because of pneumonia which subsequently healed.
In his family two brothers and four children (2 males and 2 females) apparently had the same dis-ease. The mode of inheritance was clearly of an autosomal dominant type. In all the members affected, weakness commenced in the lower limbs between the ages of 10 and 20 years.
On neurological examination after admission, there were ptosis and facial muscle atrophy, both of slight degree. There was no ophthalmoplegia. The upper and lower limbs showed diffuse muscular atrophy with a slight tendency of distal-dominant distribution. All the tendon reflexes were absent. Fasciculation and myotonia were not found. Sen-sation was normal. He was able to walk unaided. His intelligence was normal.
Laboratory studies showed normal serum CPK value. Urinary creatine was elevated (104 mg/day) with lowering of creatinine index. Electroencepha-lograms showed a slight increase in slow waves.
Electromyography revealed widespread myopathic features, except for vastus medials and biceps brachii muscles in which high amplitude potentials and an insufficient interference were observed in addition to low amplitude potentials of short dur-ation, indicating a mixed pattern. Motor nerve conduction velocities of the ulnar and tibial nerves were normal, but sensory nerve conduction velocity of the sural nerve was decreased to 37.7 m/sec.
A muscle biopsy was performed on the left per-oneus. Conventional light microscopy revealed thatabout 70% of muscle fibers, 30-50g in diameter, had one or more centrally-placed internal nuclei that were frequently surrounded by a clear space, the diameter of which approximately 1 to 20μ. Glycogen was present in the perinuclear zone on PAS staining. No target fibers or regenerating myofibers were found.
On histochemical staining of DPNH-tetrazorium reductase, no reaction or sometimes an intense reaction was observed in the central zone. Cito-architectial aberrations suggesting suggesting a degenerative process were detected in peripheral as well as central areas of muscle fibers. Differentiation of muscle fibers into two types was not clear. The poor differentiation was noted also on staining of myosin ATPase and phosphorylase, the reactions to which were deficient in the centralpart of most fibers.
Electron microscopy readily demonstrated the perinuclear region devoid of myofibrils, in which sparse amorphous material as well as mitochondria and empty vesicles were observed. Most myofibers were well preserved, but in part there were focal disorganization of myofilaments and streaming of Z-disks. In some fibers there were lipid body, myelin figure as well as well as accumulation of glycogen or mitochondria.
Among 15 cases of myotubular myopathy reported in Japan, this case showed the latest onset of the myopathy with a mild progressive course. This is the first reported case in Japan with obvious auto-somal dominant inheritance.
Copyright © 1980, Igaku-Shoin Ltd. All rights reserved.

