Japanese
English
- 有料閲覧
- Abstract 文献概要
- 1ページ目 Look Inside
肥大型心筋症(HCM)の特微的な血行動態異常は左室流入障害であり,安静時の左心収縮能は一般にむしろ亢進状態にあるとされている1)。しかし本症患者では労作時に呼吸困難,胸痛,ST下降をきたすことが少なくなく2),また突然死も労作に伴いしばしば発生する3,4)。したがって,HCMでも運動中には左心機能障害をきたすことが推測され,戸嶋ら5)やLosseら6)は本症患者の中には運動中に肺動脈平均血圧または楔入圧が著明に上昇するにもかかわらず1回拍出量や1回仕事量が増加しえず左心予備能が低下した例が認められることを報告している。しかしこれらの研究では左室容量の変化は検討されておらず,運動中の左心機能低下が拡張期流入障害によるものか,左室の収縮不全によるものかは解明されていない。
一方multigate心プールシンチ法は非観血的に左室駆出分画や左室容量を把握しえ,特にくり返してこれらの指標を把握する必要がある運動時の左心動態の評価に広く応用されている7,8)。そこで本研究では心プールシンチ法を用いてHCM患者の運動中の左心動態を検討し,本症における運動中の左心機能低下の機序の解明を試み,さらにその臨床的意義について考察を加えた。
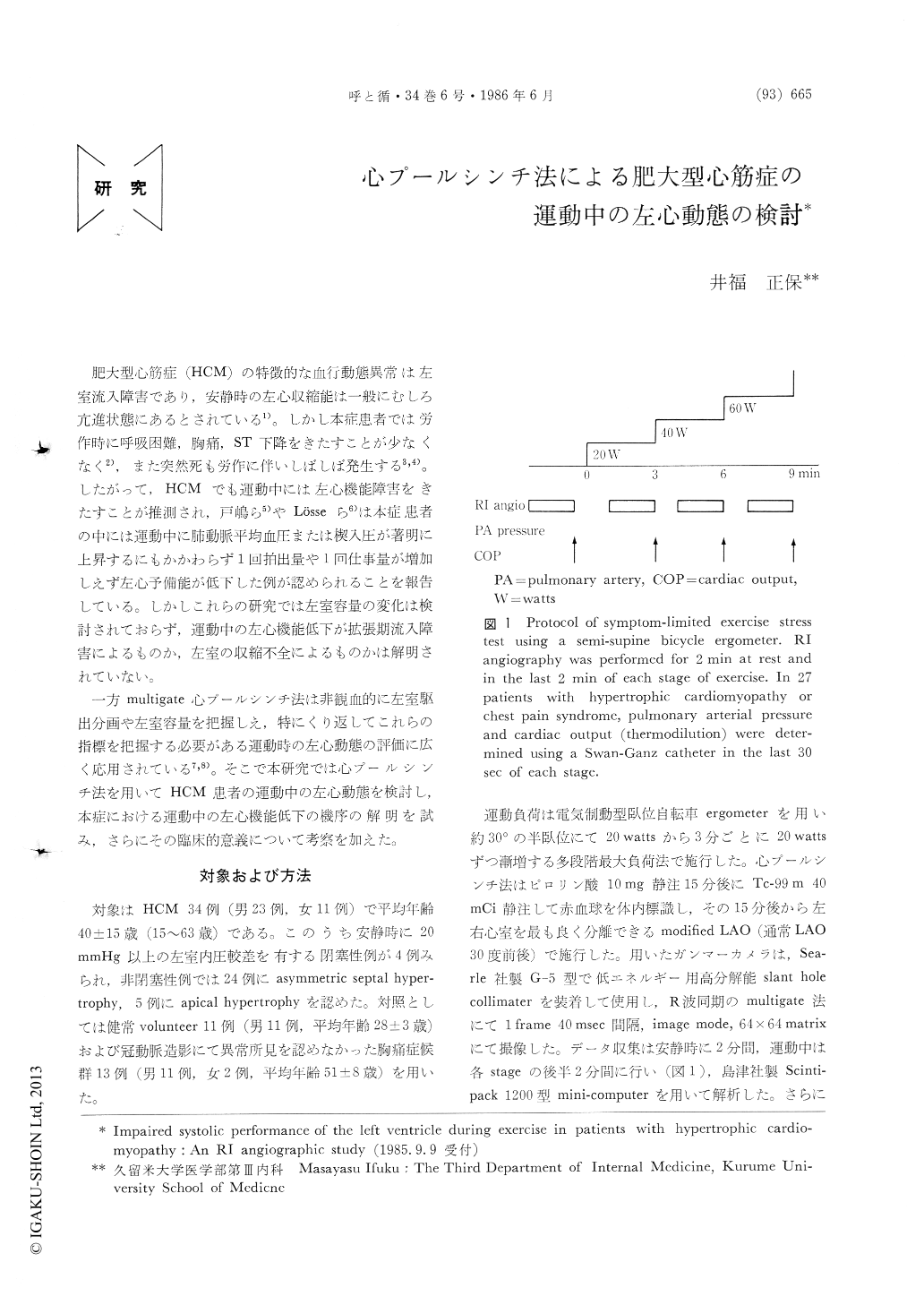
Left ventricular (LV) performance during exercise was studied using RI angiography in 34 patients with hypertropic cardiomyopathy (HCM) and the results were compared with those from 13 patients with chest pain syndrome (CP) and 11 healthy controls (C). Maximal stress test was performed using a semi-supine bicycle ergometer with an initial work load of 20W and a stepwise increase of 20W every 3 minutes. RI angiograms were taken for 2 min at rest and in the last 2 min in each step. In 20 patients with HCM and in 7 patients with CP, the pulmonary artery (PA) diastolic pressure was monitored simultaneously during exercise.
At maximal exercise, the ejection fraction (EF) and stroke volume increased by 26±16% and 6±16% in C and by 11±16% and 6±14% in CP. In contrast, they decreased by 8±15% and 7±13% in HCM, with 71% of HCM patients failing to show any increase in EF during exercise. The end-diastolic volume reduced slightly but did not differ significantly among the 3 groups. The end-systolic volume decreased by 36±17% in C and by 15±24% in CP at maximal exercise, while it remained unchanged in HCM. In addition, LV function curve shifted to right-downward and an impairment in LV systolic performance seemed to deve-lop during exercise in patients with HCM, despite an increased EF at rest. The analysis of LV diastolic per-formance revealed that the PA diastolic pressure at maximal exercise was significantly higher in HCM than in CP (18.3±5.9 vs 10.7±6.4mmHg), although the responses of the LV end-diastolic volume and of the 1/3 filling rate did not differ in these two groups. These findings suggested that exercise developed a further depression of LV compliance, but that the LV filling impairment was compromised possibly by an elevation in the filling pressure.
The present study accordingly indicates that RI angio-graphy is a valuable method in patients with HCM for assessing abnormal LV performance during exercise,which is mainly induced by depressed systolic perfor-mance.
Copyright © 1986, Igaku-Shoin Ltd. All rights reserved.

