Japanese
English
- 有料閲覧
- Abstract 文献概要
- 1ページ目 Look Inside
肥大型閉塞性心筋症(以下HOCM)と,冠動脈狭窄(以下CAD)が合併した場合,その診断,内科的・外科的治療には種々の複雑な問題が生じる。今回われわれは両者を合併した32歳男性に対しA-C bypass術を施行し良好な結果を得たので文献的考察を加え報告する。
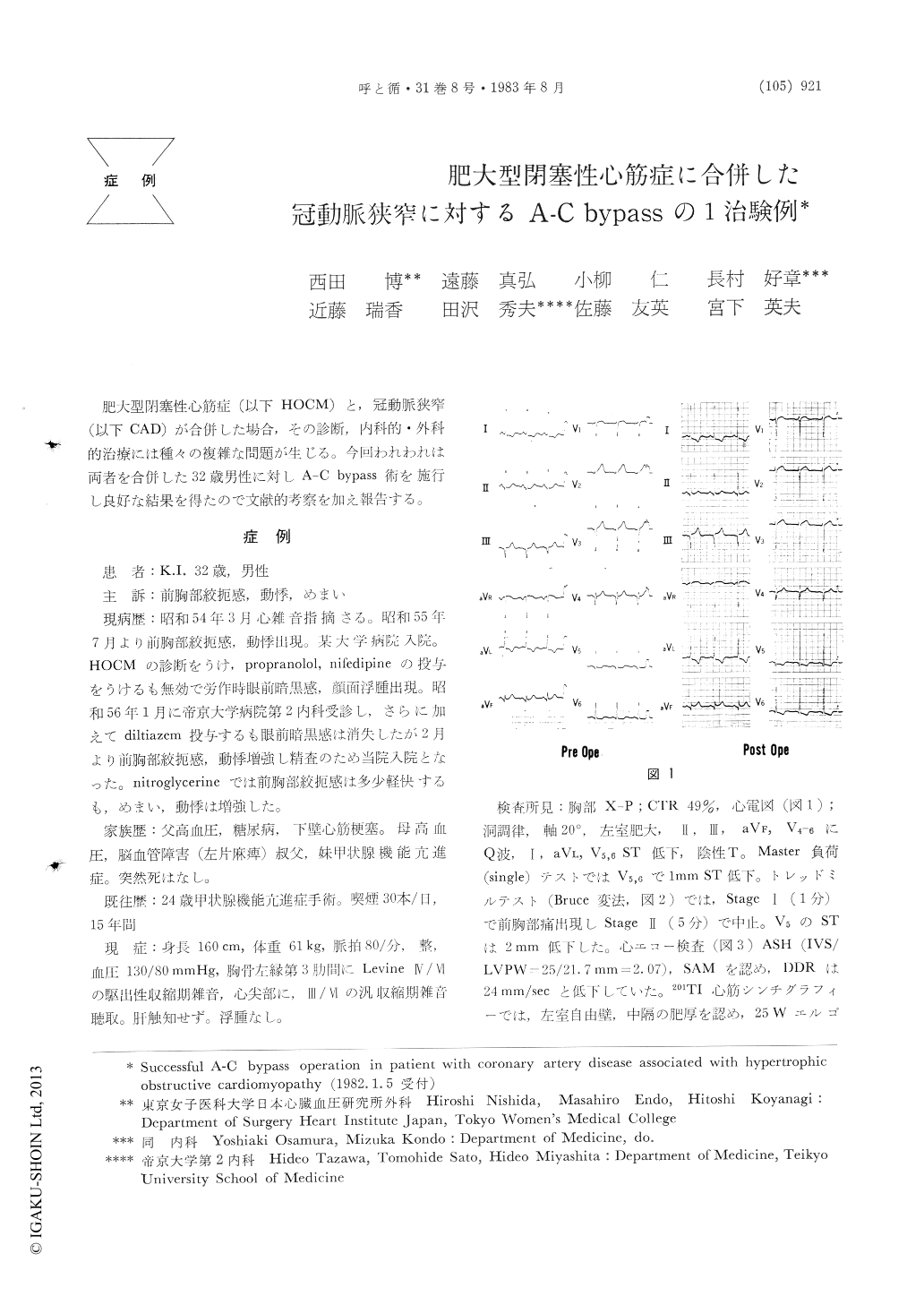
Aortocoronary (AC) bypass operation performed on a 32-years male patient who had the hyper-trophic obstructive cardiomyopathy (HOCM) treated medically is reported. He complained of precordial pain, palpitation, dizziness and black-out episodes preoperatively. These symptoms gave little response to medical treatment. At admission, 4/6 ejection murmur was audible over left 3rd ICS and 3/6 pansystolic murmur at the apex. EKG showed Q wave in II, III, aVf, and V4-6. ST-depression with inverted T was seen in leads of I, aVL, and V5,6. The treadmil exercise test showed ST-depression and occurrence of chest pain as early as at Stage I. UCG revealed the asymmetric septal hypertrophy with systolic anterior motion of the anterior mitral leaflet. Angiography demonstrated a 99% stenosis and squeezing in the proximal left anterior descend-ing coronary artery (LAD) along with a 65% stenosis in the left circumflex artery. Left ventriculography showed a so-called banana shape during systole and mild mitral regurgitation. There was the pressure gradient of 20 mmHg across the left ventricular outflow tract. Positive Brocken-brough phenomenon was observed. Biopsy of the right ventricle disclosed the bizzare myocardial hypertrophy with disorganization compatible with HOCM.
AC-bypass grafting was performed onto the LAD lesion. That of the circumflex artery and HOCM were left intact. His postoperative course was uneventful. Propranolol was administered, and the major preoperative symptoms disappeared. Exercise tolerance was also significantly improved. Coronary angiography 1 month following the procedure confirmed patency of the grafted saphenous vein. The satisfactory result in this particular case supports the accepted concept that the prognosis of HOCM is primarily related to the pathohistol-ogic severity of the diseased myocardium, and least affected by the intraventricular pressure. Surgical relief of the pressure gradient may improve symptoms, but the resultant prolonged ischemic arrest is likely to cause irreversible myocardial damage. Hence, we think that AC-bypass should be performed, if indicated, in patient with coronary artery disease associated with HOCM.
Copyright © 1983, Igaku-Shoin Ltd. All rights reserved.

