Japanese
English
- 有料閲覧
- Abstract 文献概要
- 1ページ目 Look Inside
はじめに
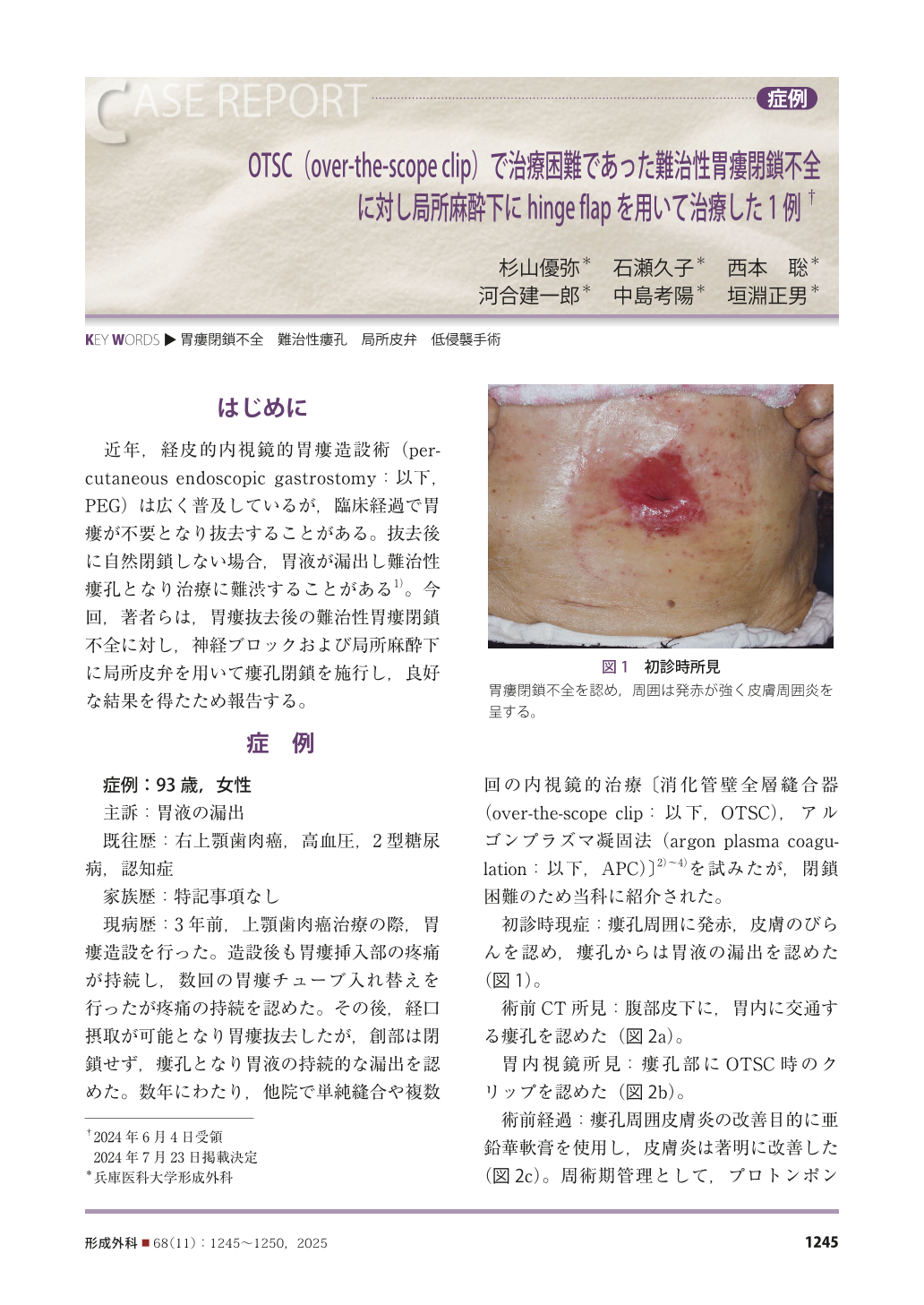
近年,経皮的内視鏡的胃瘻造設術(percutaneous endoscopic gastrostomy:以下,PEG)は広く普及しているが,臨床経過で胃瘻が不要となり抜去することがある。抜去後に自然閉鎖しない場合,胃液が漏出し難治性瘻孔となり治療に難渋することがある 1)。今回,著者らは,胃瘻抜去後の難治性胃瘻閉鎖不全に対し,神経ブロックおよび局所麻酔下に局所皮弁を用いて瘻孔閉鎖を施行し,良好な結果を得たため報告する。
Percutaneous endoscopic gastrostomy (PEG) is widely used for nutritional management. When the gastrostomy is no longer needed, the gastrostomy tube is removed. The gastrocutaneous fistula left by the gastrostomy tube usually closes on its own, but in some cases the fistula remains open. Endoscopic treatments such as an over-the-scope clip (OTSC) have been applied in cases of refractory fistulas, but if these attempts are not successful, surgical treatment is required. We present the case of a patient for whom we achieved good results by using a local flap, providing a minimally invasive fistula closure.
The patient was a 93-year-old woman who had undergone gastrostomy placement for the treatment of maxillary gingival cancer. She was able to take food orally postoperatively, and the gastrostomy tube was removed. The fistula did not close, and gastric juice continued to leak. After several endoscopic treatment attempts without improvement, we were able to close the fistula by applying a local flap under nerve block and local anesthesia. A local flap consisting of skin and subcutaneous tissue was raised as a hinge flap from the left side of the fistula. This flap was de-epithelialized.
This case indicates that our method can be performed even in elderly patients and those with poor general conditions, and it could be a helpful treatment for refractory fistula-closure failures that are difficult to treat endoscopically.
Copyright© 2025 KOKUSEIDO CO., LTD. All Rights Reserved.

