Japanese
English
- 有料閲覧
- Abstract 文献概要
- 1ページ目 Look Inside
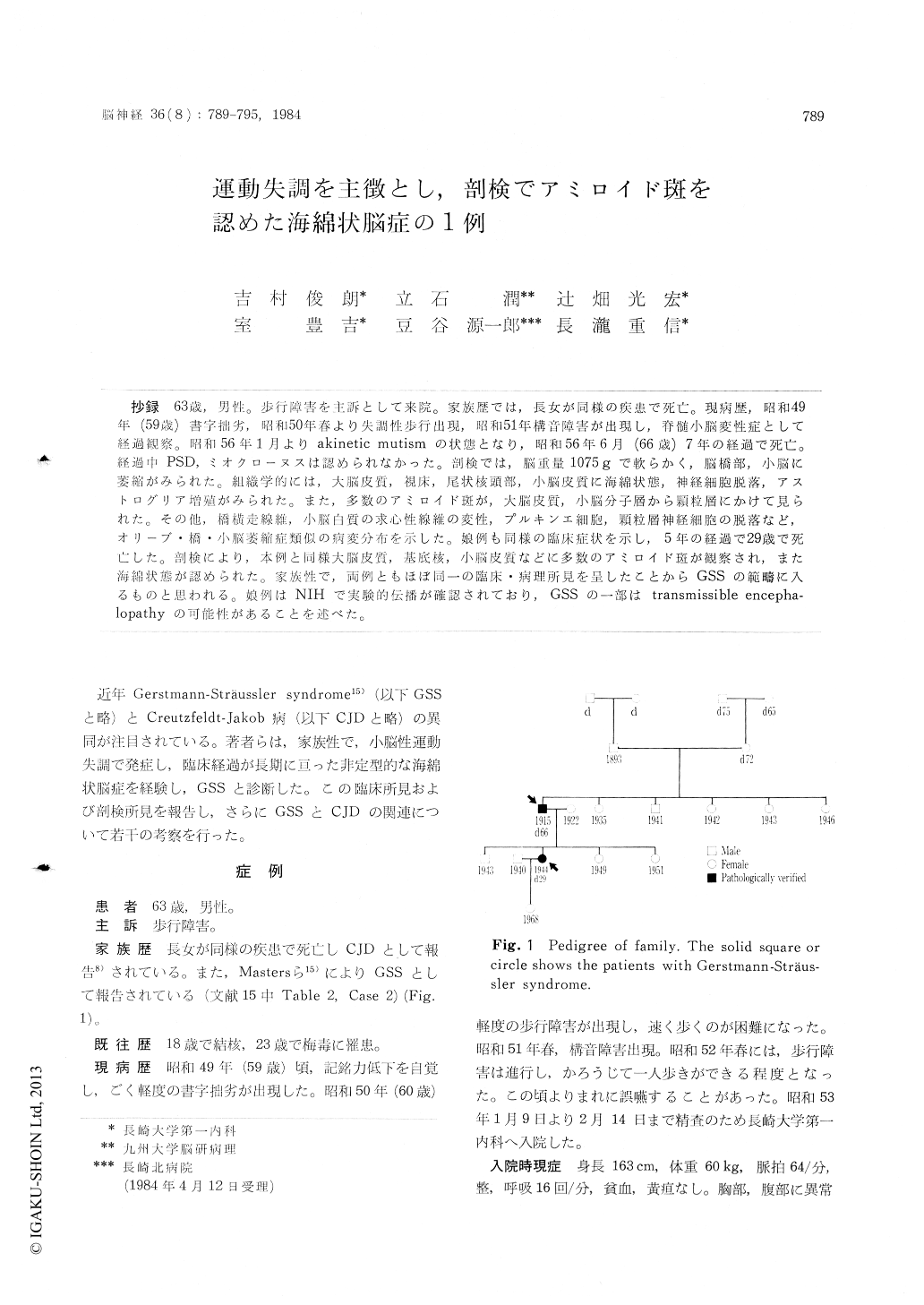
抄録 63歳,男性。歩行障害を主訴として来院。家族歴では,長女が同様の疾患で死亡。現病歴,昭和49年(59歳)書字拙劣,昭和50年春より失調性歩行出現,昭和51年構音障害が出現し,脊髄小脳変性症として経過観察。昭和56年1月よりakinetic mutismの状態となり,昭和56年6月(66歳)7年の経過で死亡。経過中PSD,ミオクローヌスは認められなかった。剖検では,脳重量1075gで軟らかく,脳橋部,小脳に萎縮がみられた。組織学的には,大脳皮質,視床,尾状核頭部,小脳皮質に海綿状態,神経細胞脱落,アストログリア増殖がみられた。また,多数のアミロイド斑が,大脳皮質,小脳分子層から顆粒層にかけて見られた。その他,橋横走線維,小脳白質の求心性線維の変性,プルキンエ細胞,顆粒層神経細胞の脱落など,オリーブ・橋・小脳萎縮症類似の病変分布を示した。娘例も同様の臨床症状を示し,5年の経過で29歳で死亡した。剖検により,本例と同様大脳皮質,基底核,小脳皮質などに多数のアミロイド斑が観察され,また海綿状態が認められた。家族性で,両例ともほぼ同一の臨床・病理所見を呈したことからGSSの範疇に入るものと思われる。娘例はNIHで実験的伝播が確認されており,GSSの一部はtransmissible encepha—lopathyの可能性があることを述べた。
Case : A 63-year-old man was admitted to our hospital because of gait disturbance. His daughter died of the same disorder at age 29. In 1974, at age 59, the patient noticed mild recent memory disturbance and clumsiness in handwriting. In 1976, his gait was markedly unstable, but he could walk without assistance, and his speech became dysarthric. In spring,1977, he was unable to walk without assistance. From Jan. 9, 1978, through Feb.14,1978, he was hospitalized in our hospital. Neurological examination revealed an ataxic gait and scanning speech. Deep tendon reflexes of the upper extremites and ankle jerks were normal, but knee jerks were absent. Pathological reflexes were not elicited. Both superficial and deep sensa-tions were normal. He was alert and showed no overt dementia. Laboratory data including CSF, EEG and brain CT were normal except positive TPHA in serum. Thereafter, he was followed up with the diagnosis of spinocerebellar degeneration. In 1979, he developed a limb ataxia. In spring, 1980, he became very irritable and was easily excited. He gradually developed dementia and uri-nary incontinence. In 1981, his illness progressed to an akinetic mutism and died of pneumonia on July 19,1981. Myoclonus and periodic synchronous discharges in EEG were not observed until his death.
The brain was 1,075g in weight after froma-lin fixation and the cerebrum was generally soft. The gyri showed no evidence of abnormalities or atrophy, while the cerebellum and brain stem, especially the pons, were atrophic. The arterial and venous systems showed no remarkable chan-ges. The spinal cord was externally unremarkable. The ventricles were dilated. The cerebral cortex, white matter and thalamus revealed a mild atrophy.The basal ganglia was almost normal. The cere-bellar hemispheres and vermis were diffusely soft and atrophic. But the dentate nuclei were well preserved.
Histologically, there were severe status spongi-osus, proliferation of astrocytes and loss of nerve cells in the cerebral cortex, thalamus and head of the caudate nuclei. The transverse fibers of the pons and the centripetal fibers of the cerebellar white matter were degenerated. In the cerebel-lum, there was a mild to moderate decrease in number and degeneration of Purkinje cells and granule cells and gliosis. There were numerous amyloid plaques which showed various morpholo-gical forms in the cerebellar cortex, cerebral cor-tex, thalamus and basal ganglia.
The histological findings, including amyloid pla-ques and status spongiosus with softening foci in the white matter of his daughter's brain, were very similar to this patient. Transmission was succeeded by inoculating the daughter's brain tissue into a monkey.
Judging from the familial occurrence, cerebellar ataxia, long clinical course and extensive amyloid plaque deposition throughout the central nervous system, both patients were diagnosed to be a Gerstmann-Straussler syndrome.
It was discussed that some patients with GSS will belong to a transmissible encephalopathy.
Copyright © 1984, Igaku-Shoin Ltd. All rights reserved.

