Japanese
English
- 有料閲覧
- Abstract 文献概要
- 1ページ目 Look Inside
「失調症状とアミロイド斑を伴う海綿状脳症(SEA)」がCreutzfeldt-Jakob病(CJD)のひとつの亜型である可能性を筆者は1981年に指摘した14)が,最近ではGerstmann-Sträussler-Scheinker病(GSSD)とSEAの関連が注目されている。筆者はCJDを臨床病理学的にひとつの「症候群」として把握している14,16)が,本論文ではCJDにおけるSEAの位置づけについて,pancncephalopathy型CJD(PE-CJD)を中心に他の亜型との関係を明らかにしながら論ずることにする。なおCJDの神経病理は筆者の論文,総説を参照されたい16,17)。
This paper shows that "spongiform encephalopathy with ataxia and amyloid plaque (SEA)" is a clinicopathologically distinctive subtype of Creutzfeldt-Jakob disease (CJD). SEA is characterized by unique clinical feature simulating cerebellar ataxia and neuropathological change similar to the panencephalopathic type of CJD (PE-CJD). SEA seems to be prevailing in Japanese up to date, at least.
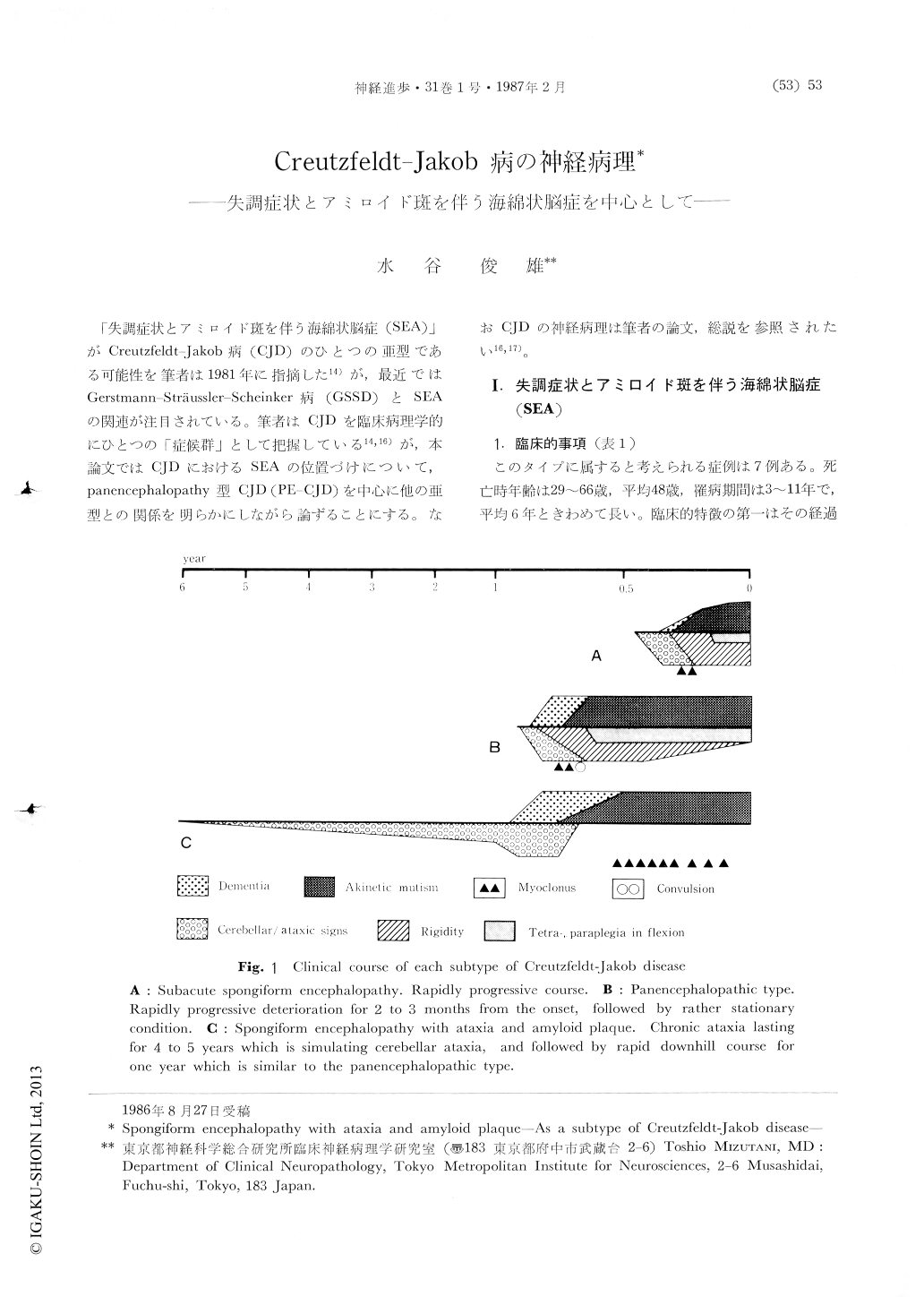
The clinical course is quite characteristic. The total duration of illness ranges from 3 to 11 years, the mean being 6. The most part of the total clinical course is progressive ataxia, and the final stage shows rapid downhill! course of mental function. The disease starts with ataxia which is gradually worsening for 4 to 5 years. For this reason, the initial clinical diagnosis is olivopontocerebellar atrophy, or hereditary ataxia, especially when similar features are observed in the siblings or relatives. At the final stage for about one year, however, dementia resulting into akinetic mutism rapidly appears, and thus, CJD is suspected at last. The clinical signs, which are unusual in typical CJD, are hypotonia even at the last stage and hyporeflexia, while myoclonus and other involuntary movements, and rigidity are rare in SEA. The neuropathology is as follows. 1) Kuru or Kuru-like plaques are scattered in the cerebellar cortex, cerebral cortex, basal ganglia and even the white matter. It is remarked that the dendrites of Purkinje cell within the plaque are thickened and deformed, although it is said that Kuru plaque is different from senile plaque in the absence of degenerated neurites. 2) Diffuse degeneration of the white matter, which frequently is more predominant than the cortical spongy state, occurs in the centrum semiovale, frontal and temporal lobes, and corpus callosum. However, the internal capsule is usually spared from the change. The circumscribed spongy necrotic foci, which are the most characteristic of PE-CJD, are not found. 3)Neuronal inflation is found extensively in the deeper layers of the cerebral cortex, brainstem motor nuclei, inferior olive and anterior horn of the spinal cord. Neuronal vacuolation also is found particularly in the brainstem motor nuclei, substantia nigra, inferior olive and anterior horn. 4) Primary thalamic degeneration characterized by severe neuronal loss and fibrillary gliosis occurs. 5) Loss of both Purkinje and granule cells in the cerebellar cortex is found in varying degrees from case to case. The cerebellar cortical degeneration of granule cell type is never found. 6) Axonal swellings are frequently found in the pontine base, inferior olive, dentate nucleus and substantia nigra. 7) Combined degeneration of the posterior column, spinocerebellar and corticospinal tracts is found.
Copyright © 1987, Igaku-Shoin Ltd. All rights reserved.

