Japanese
English
- 有料閲覧
- Abstract 文献概要
- 1ページ目 Look Inside
I.緒言
頭部外傷や脳内出血などの脳血管障害あるいは術後の脳浮随や後出血などによる,急性の頭蓋内圧亢進の状態は,それが容易に天幕切痕ヘルニアや大後頭孔ヘルニアを惹起することにより,直接生命の予後と結びついているだけに,脳神経外科領域においては,早急にその解決の望まれる重大な問題である。その解決のために,頭蓋内圧亢進の原因となる浮腫や出血についての研究は,かなり広汎に行なわれているが,このような状態のときに,頭蓋内圧の高さがどの位あるものであるか,また,浮腫や出血が発生したために,頭蓋内圧がどのような推移を示すかなどの点についてはまったく知られていない。これは,ひとつには,臨床例において,頭蓋内圧を,安全,容易に,持続的に,長時間に計測記録する方法がなかったためであると考えられる。
われわれは12)13),最近,臨床例において,安全,容易に,長時間にわたつて持続的に頭蓋内圧を計測記録する方法を発表してきたが,今回は本法によつて,術後の頭蓋内圧を検討してみた結果,頭蓋内出血や脳浮腫発生の時期,また,これらの頭蓋内圧に及ぼす影響などについて若干の新知見を得たので報告する。
In order to solve the problems concerning intracranial hypertension of various causes such as brain tumors, cerebral traumas, cerebrovascular diseases, and cerebral edema caused by various pathological conditions, it is absolutely necessary to know accurate intracranial pressure dynamics. For this purpose, various methods have been tried in the past, but there has never been a satisfactory way of knowing the accurate intracranial pressure continuously for long period of time. Con-tinuous recording of ventricular fluid pressure using a strain-gage pressure transducer satisfies our require-ments to a certain extent. However, in order to transmit the intracranial pressure, the ventricular fluid must be led to the transducer head through a catheter. And therefore, the entire set up, including the trans-ducer head must he kept sterile. This is not only quite a nuisance but also sometimes dangerous. Fur-thermore, in order to continue the recording, free communication of cerebrospinal fluid between the ven-tricle and the transducer must always be maintained. This is quite a difficult problem when severe cerebral edema developes and as the result the ventricle beco-mes collapsed. Also, when the ventricle is shifted way over to the other side by a hematoma or other space taking lesions, it is difficult to maintain the communi-cation through the catheter in the ventricle. Finally, using this method, it is not possible to record the pres-sure in the posterior fossa.
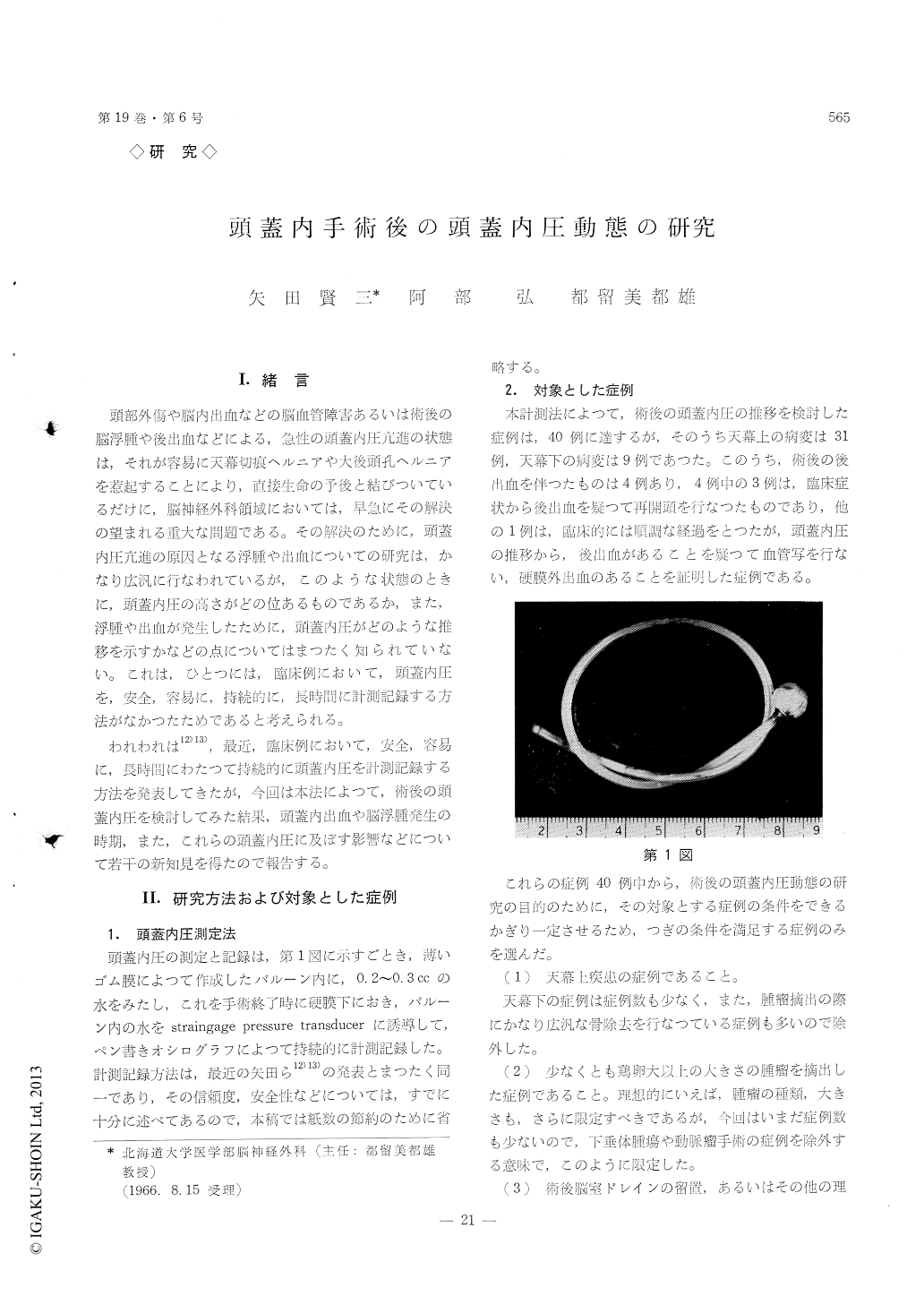
In order to solve these problems, we have designed a small rubber bag with 7mm diameter. The wall of the bag is made thin enough to transmit the intra-cranial pressure through this wall to the fluid inside the bag. The bag is placed under the Jura, and the fluid inside is connected to a strain-gage pressure trans-ducer through a catheter with 2 mm diameter. The catheter is designed soft enough not to traumatize the cerebral tissue but hard enough to be tied to the skin edge with a suture material without being col-lapsed. The bag is placed under the Jura after being inflate with 0.2cc of water at the time of closure of the Jura. Since the content of the bag is separated from the intracranial content by the rubber wall, after closure of the skin, the catheter can be connected to the transducer without using a sterlile technique. The pressure is recorded continuously by using an ink-writing oscillograph. After the end of recording, the content of the bag is drained, and the bag can he pulled out easily just as in case of ventricular catheter. Using this method, we have made intracranial pressure recordings on 39 post-operative cases. There was one complication, that was a bacterial meningitis caused by breaking of the bag. After this accident, the wall of the bag was made double and has never been a complication since. The recordings were continued for 2 clays to as long as 3 weeks. When the recording is made postoperatively, postoperative care following in-tracranial surgery becomes much easier than the con-ventional method such as observation of the level of consciousness, size and reaction of the pupils, blood pressure and pulse. By observing the intracranial pressure it is extremely easy to find postoperative hemorrhage long before the classical clinical signs be-come evident, as in the cases with postoperative hemorrhaage, the pressure elevates quite steeply fol-lowing the end of surgery and it reaches to 600~700 mm H2O within 2~3 hours. In cases of without com-plications, the pressure gradually elevates after sur-gery and reaches to its first plateau at about 12 hours. The pressure then gradually decrease or re-elevates at about 26~48 hours. If postoperative cerebral edema develops, the course of the elevation takes much more the same way as in cases without complications but the degree of elevation is more marked than the other.
We believe this method is easy and safe enough for clinical use, and therefore it should be used rou-tinely for easier and safer postoperative care follwing intracranial surgery.
Copyright © 1967, Igaku-Shoin Ltd. All rights reserved.

