Japanese
English
- 有料閲覧
- Abstract 文献概要
- 1ページ目 Look Inside
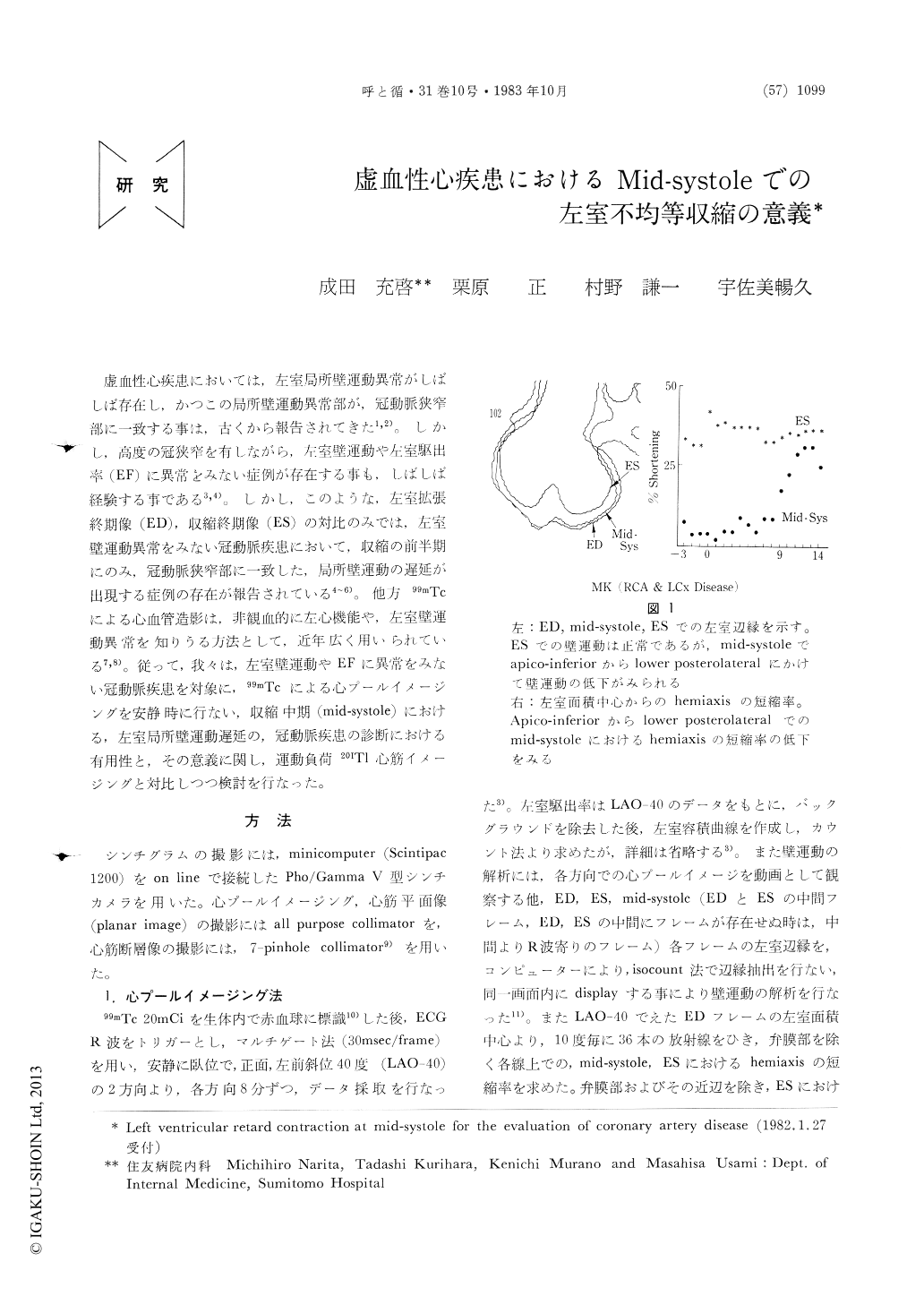
虚血性心疾患においては,左室局所壁運動異常がしばしば存在し,かつこの局所壁運動異常部が,冠動脈狭窄部に一致する事は,古くから報告されてきた1,2)。しかし,高度の冠狭窄を有しながら,左室壁運動や左室駆出率(EF)に異常をみない症例が存在する事も,しばしば経験する事である3,4)。しかし,このような,左室拡張終期像(ED),収縮終期像(ES)の対比のみでは,左室壁運動異常をみない冠動脈疾患において,収縮の前半期にのみ,冠動脈狭窄部に一致した,局所壁運動の遅延が出現する症例の存在が報告されている4〜6)。他方99mTcによる心血管造影は,非観血的に左心機能や,左室壁運動異常を知りうる方法として,近年広く用いられている7,8)。従って,我々は,左室壁運動やEFに異常を入ない冠動脈疾患を対象に,99mTcによる心プールイメージングを安静時に行ない,収縮中期(mid-systole)における,左室局所壁運動遅延の,冠動脈疾患の診断における有用性と,その意義に関し,運動負荷201Tl心筋イメージングと対比しつつ検討を行なった。
Regional left ventricular (LV) wall motion abnormality (retard contraction) at mid-systole was examined in 17 patients with coronary artery disease (CAD) with normal LV ejection fraction (≧55%) and normal holosystolic wall motion, and in 10 normal subjects. CAD group consisted of 3 patients with old myocardial infarction (OMI) and 14 patients with effort angina (EA).
After red blood cells were labeled with 20mCi of Tc-99m in vivo, R-wave triggered multiple-gated cardiac blood pool imaging was obtained at anterior and 40-degree left anterior oblique position at rest. LV perimeter was detected automatically by iso-count method. In 16 patients with CAD, exercise stress myocardial perfusion imaging (MPI) with TI-201 was obtained both at immediately after the exercise stress (initial) and 3 hours after the exercise stress (delayed).
In normal subjects, wall motion at mid-systole was uniform. On the contrary, in 10 patients with CAD regional retard contraction at mid-systole was observed (59%) and the loci of retard contraction were coincided well with the site of coronary artery stenosis and perfusion defect at initial Tl images.
Out of 10 patients, in whom retard contraction at mid-systole was observed, 5 patients with EA showed incomplete obliteration of initial defect at delayed MPI and 2 patients with OMI showed persistent defect. On the other hand, 7 patients with CAD showed normal wall motion at mid-systole, and in 6 of them exercise stress MPI showed complete obliteration of initial defect but one patient with OMI showed no perfusion abnormality. Besides there were 4 patients of EA who experienc-ed prolonged anginal pain (more than 20 minutes) without electrocardiographic evidence of MI, and they all showed retard contraction at mid-systole.
These facts indicated the existence of small necrisis at retard-contracted myocardial segments.
In conclusion, the study of wall motion abnormality at mid-systole is useful to detect the site of coronary artery stenosis in patients with CAD with normal holosystolic LV function, and retard contraction at mid-systole suggested the existence of small necrosis at that segment.
Copyright © 1983, Igaku-Shoin Ltd. All rights reserved.

