Japanese
English
- 有料閲覧
- Abstract 文献概要
- 1ページ目 Look Inside
I.緒言
Merrittの成書によると,後頭蓋窩におけるmeningiomaは比較的稀で頭蓋内meningioma例のうち5%程度であるという1)。また小脳橋角部に発生する腫瘍のうちmeningiomaは5〜6.3%位という報告もある2)4)。さらに顔面神経麻痺が徐々に進行するものでは腫瘍によるものを考えるべきであるという3)。今回顔面痙攣を初発症状とし4年間で一側高度の顔面神経麻痺を来たした例で精査した結果,後頭蓋窩に巨大なmeningiomaを認め得たので報告し参考に供した。
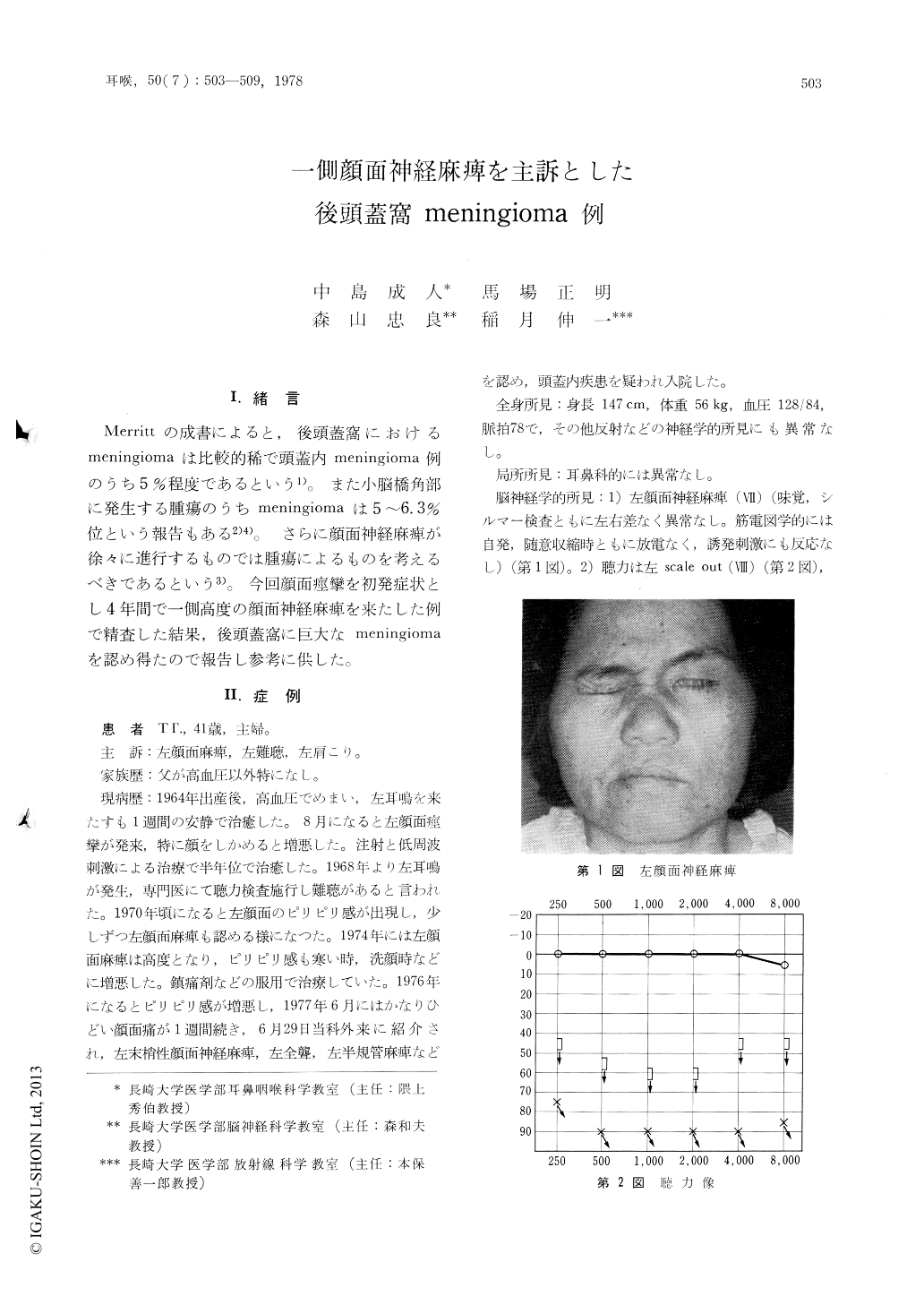
A 41-year-old housewife complained of a gradually progressive facial palsy of 4 years' duration, deafness, intermittent facial pain and strain of the left shoulder. Neurootological examinationsrevealed total deafness, canal paresis in the left ear and no response of body sway to galvanic stimulation of the left side, and slight disturbance of optokinetic nystagmus to the right. Slight paralysis of IX, XI and XII cranial nerves was recognized, but no other neurological signs were noted. Electromyographic findings of the left facial muscles showed no response in voluntary and evoked movement. Electroencephalography demonstrated an abnormal slow wave focussed at the left parietotemporal region. Electrocochleography showed aretrocochlear lesion. CT scan and angiography (CAG, VAG) revealed a large tumor growing to the middle fossa from the posterior fossa of the left side. Since the tumor was adherent to the base of skull and the petrous bone, subtotal resection was performed and the tumor was confirmed as meningioma (spindle cell type) histologically. The author discussed about the differential diagnosis of tumors at the cerebellopontine angle, especially neuromas of the acoustic, facial and trigeminal nerves, and intracanalicular hemangioma.
Copyright © 1978, Igaku-Shoin Ltd. All rights reserved.

