Japanese
English
- 有料閲覧
- Abstract 文献概要
- 1ページ目 Look Inside
Ι.はじめに
Anterior transcallosal approach(ATA)により,第3脳室部病変を手術する場合,自然孔(Monro孔)を通した術野だけでは根治術が望めないことも多く,脳弓間もしくはMonro孔を広げる様々な工夫が必要とされる.それぞれの方法に一長一短があるように思われるが,詳細に記述されたものは意外に少ない6,12).われわれは,主にchoroidal fissureを利したsub/transchoroidal approachを用いて手術をを行ってきたが,その有用性と共に,いくつかの問題点を実感した.そこでこれらの適応と限界につき,われわれの経験を元に考察を加える.
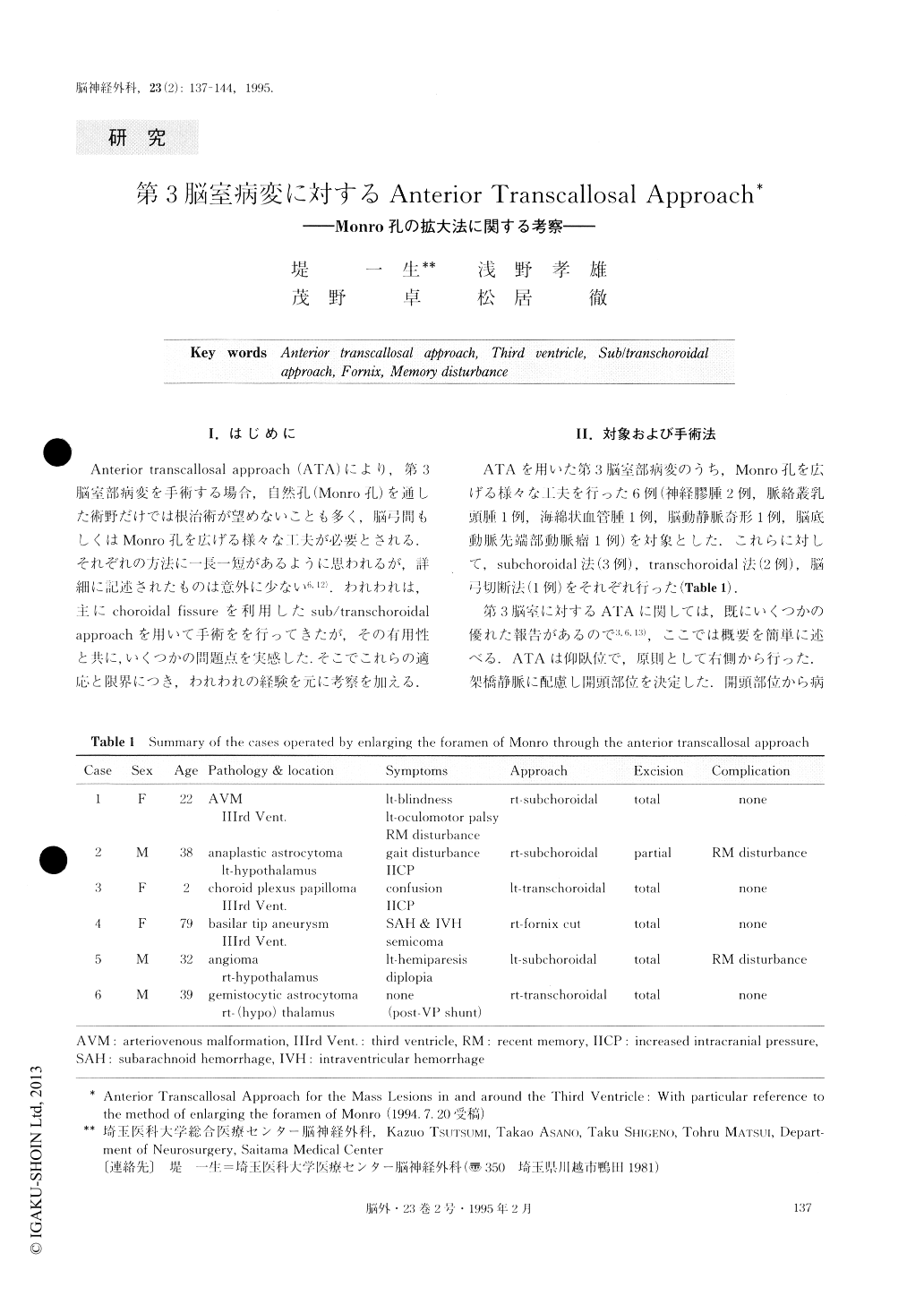
Enlargement of the foramen of Monro is an essential maneuver to obtain an appropriate surgical view when large, solid lesions in and around the third ventricle are to be removed via the anterior transcallosal approach (ATA). For this purpose, three methods, i.e., the sub-choroidal, transchororidal, and transfornicial approaches have so far been reported. However, since the locations and the pathological natures of space occupying lesions in this region are widely variable, the indication as well as the feasibility of each approach has remained rather unclear. The present paper deals with our surgical ex-perience with six patients (2 gliomas, 1 angioma, 1 AVM, 1 plexus papilloma, 1 basilar top aneurysm) operated on using the ATA in which variable methodsof enlarging the foramen of Monro were employed. Aiming at complete removal or clipping of the lesion, the seemingly best among the above three approaches was determined preoperatively, considering the size, location, and pathological nature of the lesion. The shape of the choroid plexus of the roof of the HIrd ventricle as revealed by MRI was also taken into account. The subchoroidal, transchoroidal, and the trans-fornicial approaches were employed in 3, 2, and 1 cases, respectively. Except for one glioma which ended up being removed extensively, all the tumors and AVM were totally removed and the aneurysm successfully clipped. From the above experience, the merits and de-merits of each approach for different types of lesions are discussed in view of their suitability for achieving total removal. Importantly, however, we encountered a major postoperative complication i.e., the disturbance in recent memory, which occurred in two of the three pa-tients who had normal memory preoperatively. These two patients had hypothalamic tumors operated on by the subchoroidal approach from the intact side. By con-trast, no complication was detected in another hypotha-lamic glioma operated by the same approach from the lesion side. This discrepancy is considered to be due to the following reason. Since memory disturbance occurs only when the relevant structures in and around the thalamus are bilaterally affected, it is not manifest in the unilateral lesion, even if the structures are irrevers-ibly damaged by intraaxial lesions such as glioma. In such a condition, even slight damage to the contralater-al thalamus can lead to the occurrence of memory dis-turbance. Even if maximal precautions were exercised, some damage to the thalamus due to retraction and obliteration of small arteries and veins is unavoidable when the sub- or trans-choroidal approach is carried out. From our experience, therefore, it seems advisable not to carry out these approaches from the contralateral side, particulary when the lesion is intraaxial. All the three approaches otherwise yielded satisfactory results, when the indication for each was thoroughly examined preoperatively.
Copyright © 1995, Igaku-Shoin Ltd. All rights reserved.

