Japanese
English
- 有料閲覧
- Abstract 文献概要
- 1ページ目 Look Inside
I.はじめに
下垂体前葉のホルモン非分泌性腺腫は,通常頭痛,全般的な下垂体機能低下,視力視野障害で会くつかれることが多い.しかし稀ではあるが下垂体前葉組織の炎症性病変によって同様な症状を呈することが知られている.今回われわれの経験した1症例も臨床的には,無月経と乳汁分泌が主訴で,放射線学的にはトルコ鞍内に主座をもつ鞍上部に進展した腫瘤として認められた。術前診断はホルモン非分泌性下垂体腺腫としたが,組織学的には下垂体前葉組織の虫くい状の破壊を示す他に,散在性のリンパ濾胞の形成を科三う多数のリンパ球浸潤と異物型多核巨細胞,石灰沈着を認めその周囲には類上皮細胞が集合している炎症性疾患でgranulomatous hypophysitisと診断した.本症例の発症機序として自己免疫反応の関与が示唆されていることから自己免疫疾患としての可能性を検討したが確証は得られなかった.
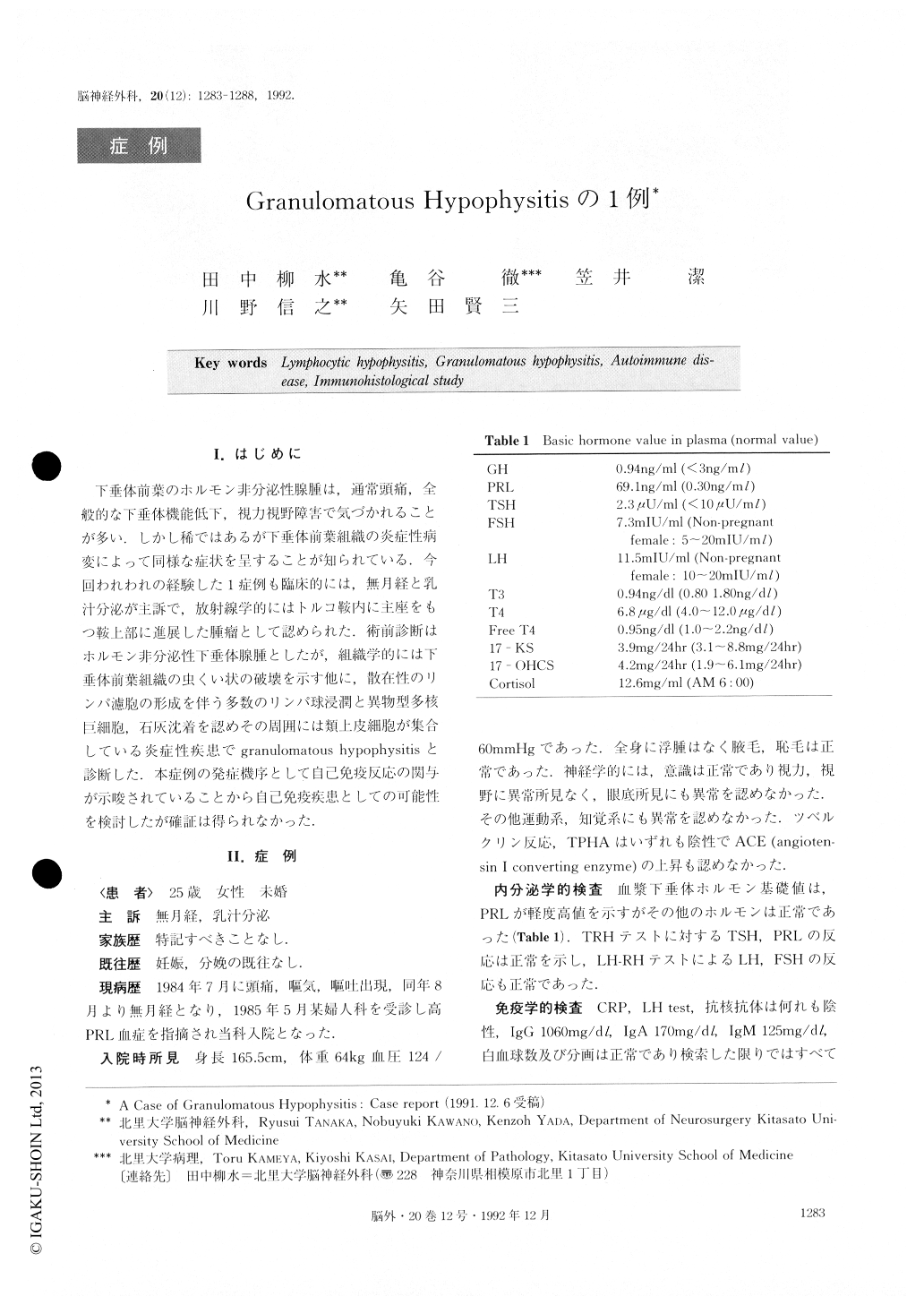
The patient was an unmarried,25-year-old womanwho presented herself with amenorrhea and lactationas her chief complaints. Radiography revealed a tumorin the sella turcica. Upon neurological examination atthe time of admission, there were no abnormal findingsaffecting the field of vision or visual acuity, and noabnormalities were seen in the fundus oculi. In endocr-nological tests, the basal plasma values of pituitary hor-mones were normal except for that of prolactin, whichwas 69.1 ng/ml. The preoperative diagnosis was non-functioning pituitary adenoma, and this neoplasm wasresected by the transsphenoidal approach. Postopera-tive histological investigation showed vermiculous de-struction of the anterior lobe of the pituitary gland, andalso scattered lymph follicles accompanyillg infiltrationby numerous lymphocytes and mu}tinucleated foreign-body giant cells, and deposition of calcium, These find-ings, together with the epithelioid cells gathered aroundthem, Pointed to adiagnosis of granulomatous hypo-physitis. The causes of granulomatous hypophysitis are known to include syphilis, tuberculosis, sarcoidosis, mycotic granuloma, and foreign-body granuloma due to the rupturing of a Rathke's cleft cyst, but no evidence of any of these was found in this patient. Another known source of .inflammatory lesions in the hypophy-sis is lymphocytic hypophysitis, which resembles Hashimoto's autoimmune disease of the thyroid gland, and which is characterized both by the formation of lymph follicles and by extensive lymphocyte infiltra-tion. In relation to the cause of granulomatous hypophysitis, thinking that it might possibly be an autoimmune disease, we conducted an immunological investigation, and also made a serological study of autoantibodies, but obtained no positive results. In addition, using the patient's serum, we carried out the indirect fluorescent antibody technique to test for the presence of autoantibodies to the cells of the anterior lobe of the pituitary gland, but were unable to detectany. However, in an immunohistological study per formed at the same time, multinucleated giant cells were confirmed by the fact that they were lysozyms stain positive and s-100 stain positive, to be a type of histiocyte, and the cytoplasm within these same giani cells was found to be positive to immunostaining with anti-GH and anti-ACTH. This points to the possibility that the normal cells of the anterior lobe of the pituit-ary gland are for some reason injured by cells that sub-sequently become histiocytic giant cells by rapidly con-suming the resulting cell fragments.
There have recently been many reports on cases of granulomatous hypophysitis which, like the present case, have been diagnosed neurosurgically, but few re-ports that collaborative studies have been conducted on its etiology, and those with nothing but speculative data are numerous.
Copyright © 1992, Igaku-Shoin Ltd. All rights reserved.

