Japanese
English
- 有料閲覧
- Abstract 文献概要
- 1ページ目 Look Inside
I.はじめに
椎骨動脈解離性動脈瘤(以下VA-DA)は,従来稀な疾患とされてきたが,放射線学的診断技術の向上と同疾患に対する関心の高まりなどにより,近年その報告が増加している.VA-DAでは,保存的療法での予後は極めて不良であり,積極的に外科的治療が行われるようになってきたが,手術に際しては椎骨動脈の結紮やtrappingを要するため,ときに血行再建術の併用が必要となる.今回われわれは,左右後下小脳動脈(以下PICA)側々吻合による血行再建を要したVA-DAの1例を経験したので報告する.
Abstract
A case is reported of ruptured dissecting aneurysm of the intracranial vertebral artery (VA) operated on with VA trapping and bilateral posterior inferior cere-bellar artery (PICA) side-to-side anastomosis.
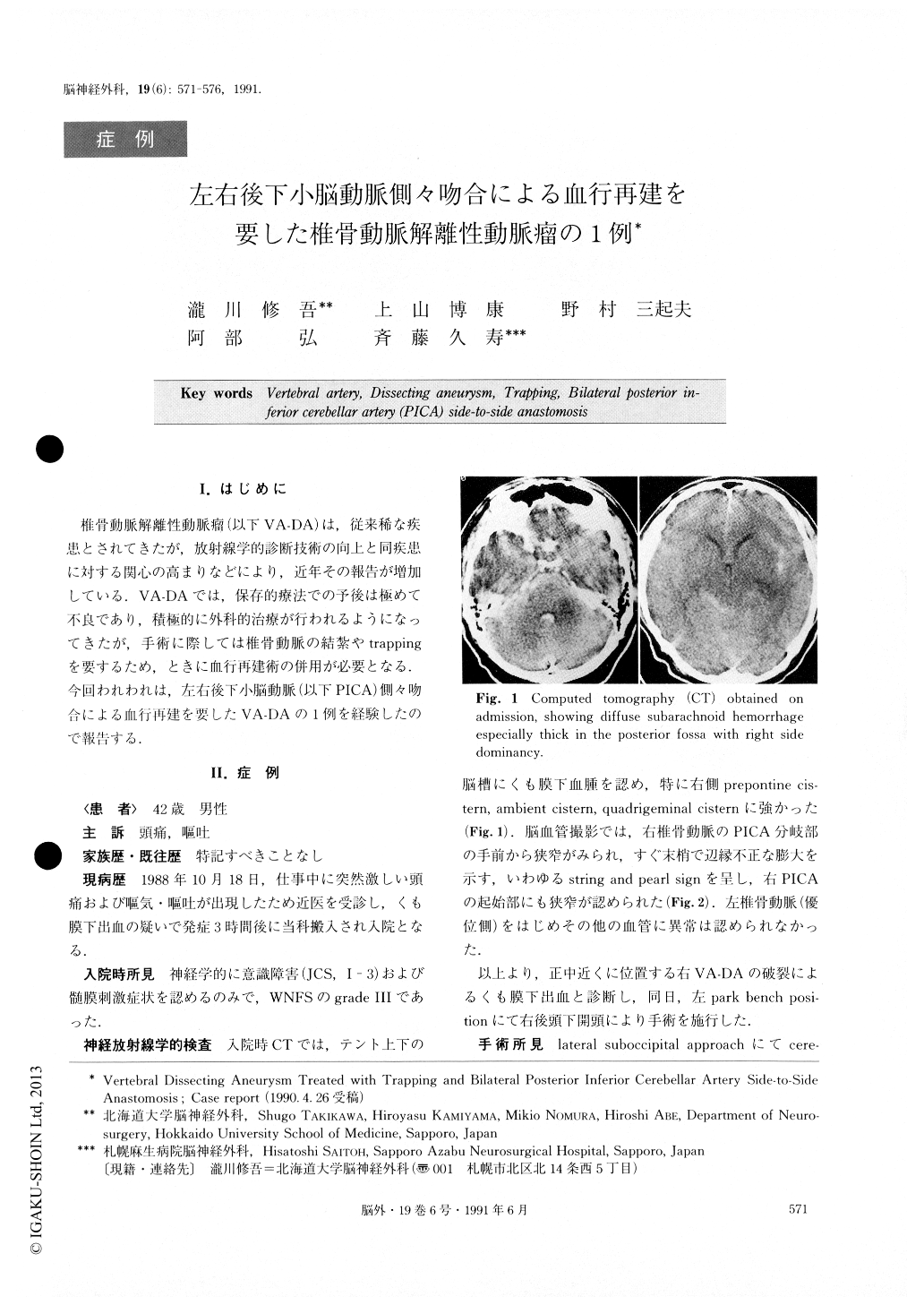
A 42-year-old male suddenly developed severe headache and vomiting. On admission, 3 hours later, he was in a state of moderate confusion (Japan Coma Scale 3) and had neck stiffness. Computed tomography (CT) revealed diffuse subarachnoid hemorrhage, espe-cially thick in the posterior fossa with right side domi-nancy. Right vertebral angiography disclosed a fusi-form dilatation with proximal narrowing of the right VA which originated just proximal to the VA-PICA junction. Lateral suboccipital craniectomy was under-taken with the patient in a left park bench position. Right VA was dilated and discolored black, and right PICA arose from the proximal portion of this aneurys-mal dilatation. Since it was impossible to clip the VA distal to the PICA for the proximal clip-occlusion, the VA including the VA-PICA junction was trapped. Con-sidering the risk of developing infarction at the PICA territory, bilateral PICA was anastomosed at their posterior medullary segment in a side-to-side fashionbecause the occipital artery (OA) had been cut at the skin incision and could not be used for the OA-PICA anastomosis. The postoperative course was benign, but a mild lateral medullary syndrome developed. CT re-vealed no abnormal low density area and left vertebral angiography demonstrated the patency of the bypass. Thereafter, the deficit subsided gradually and the pa-tient was discharged. He is presently working without neurological deficit.
As far as we know, this is the first case that has undergone PICA-PICA side-to-side anastomosis. When performing revascularization of the PICA, the OA-PICA anastomosis is thought to be the one of choice. Since an intracranial interarterial bypass such as the PICA-PICA anastomosis runs the risk of enlarging the infarction in case of unsuccessful anastomosis, it should not be attempted lightly. This operative procedure, however, might be taken into consideration by skillful surgeons when the OA cannot be used as a donor artery, as in this case. Most of VA dissecting aneurysms cannot be operated on with neck clipping and require proximal VA occlusion or trapping. There-fore, it is considered that we should always take into account the possible necessity of revascularization dur-ing the operation. If it is necessary, we should under-take it positively if there is any likelihood that ischemiamay develop because of occlusion of the parent artery.
Copyright © 1991, Igaku-Shoin Ltd. All rights reserved.

