Japanese
English
- 有料閲覧
- Abstract 文献概要
- 1ページ目 Look Inside
I.はじめに
視床は,脳血管性障害の好発部位のひとつである。視床障害の臨床症状として,視床症候群は,DéjerineおよびEgger1)によつて始めて記載され,Roussy2)にいたつて、ほぼ確立された、しかし,視床障害例の中で,明らかな視床症候群を呈するものは,比較的にまれである.視床障害が臨床的に看過されることも,少なくない。また,視床の出血,あるいは硬塞例が,非定型的な脳卒中発作例として観察される場合もある。
この研究の目的は,次の3点を解析し,考察することにある。
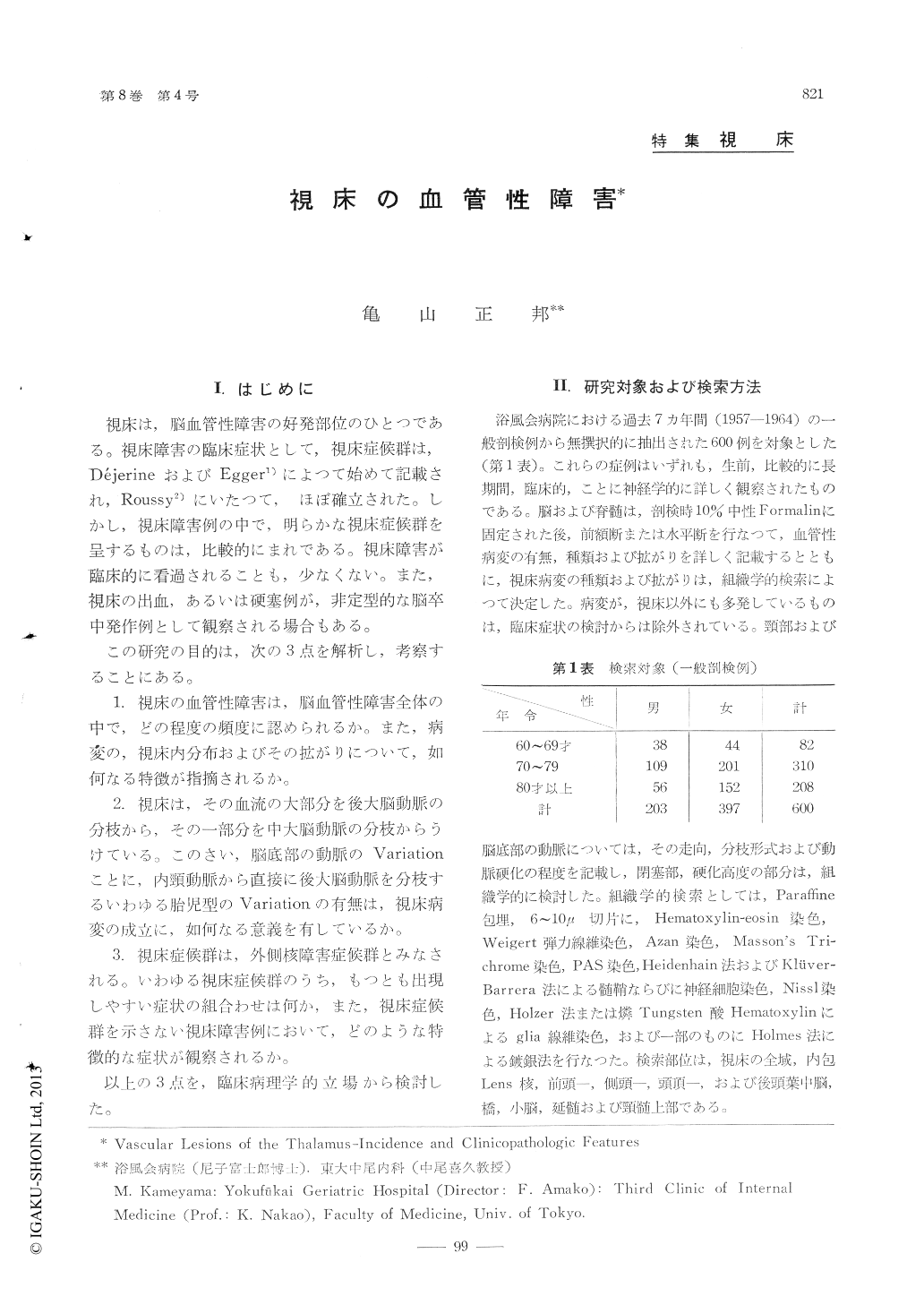
The brains of 600 cases aged sixty and overwhich had undergone routine autopsy at the Yoku-fukai Geriatric Hospital were intensively studied.The exact site and size of thalamic lesions weredetermined on histologic preparations.
1. From the practical point of view, cerebralhemorrhage and infarction were subdivided, accord-ing to their size and clinical significance, into threegroups: large (fatal within one month after theonset), medium-sized (non-fatal with clinical mani-festations), and small (less than 0.5cm. in all dim-ensions, without clinical signs). Thalamic hemorr-hage was found in 38% of "large," in 43% of"medium-sized," and in 45% of "small" groups.Infarction involved the thalamus in 0% of "lar-ge," 14% of "mediumsized," and 31% of "small"groups. About 70% of medium-sized or small tha-lamic lesions were located in the lateral nuclei.Arterial or arteriolar fibrinoid changes, regardedas an important causative vascular pathology ofcerebral hemorrhage or small infarction in hyper-tensive subjects, were most frequently seen in theposterior half of the thalamus, i. e., within theterritories of the thalmogeniculate mail thalamoperfo-rate arteries.
2. An embryonic derivation of the posteriorcerebral artery from the internal carotid was obse-rved in 37% of all cases examined. Thalamiclesions were significantly lateralized to the side ofthis variation.
3. Referable symptons of thalamic massive he-morrhage at the initial phase of a stroke were asfollows: conjugate downward deviation of eyeballs,decerebrate rigidity, severe sensory disturbanceswith slight hemiparesis and deep coma without la-terality of motor signs.
4. Thalamic syndrome was rather infrequent inits complete form. Symptoms most characteristicand most commonly observed in lateral thalamiclesions were a combination of hemiparesis, sensorydisturbances including hyperpathia, dysesthesia, loss of deep sensation, or spontaneous pain, andataxia of the upper extremity of the involved side.Patterns of sensory symptoms were discussed froma view of local diagnosis.
5. Sites of lesions responsible for central painwere most frequently found in the suprathalamic,followed by the thalamic, pontine, and corticallevels. Mechanisms of central pain were brieflydiscussed.
6. Unilateral or bilateral involvement of thelitmus, including the medial nuclei as well as thecentrum medianum, was considered on clinical andanatomical grounds with case presentations, withthe conclusion that more emphasis should he laidon thalamic lesions in interpreting the organicbasis of neuropsychiatric phenomena of senilepatients.
Copyright © 1964, Igaku-Shoin Ltd. All rights reserved.