Japanese
English
- 有料閲覧
- Abstract 文献概要
- 1ページ目 Look Inside
脳手術又は頭部外傷等の專ら機械的傷害作用が直接脳に作用し之により過高熱が現われた場合,通常躯幹は非常に熱くなるのに四肢は氷のように冷たい,而も発汗は殆んどない,意識は混濁し,高度の頻脈,頻呼吸及び呼吸困難,瞳孔の異常等が認められ.予後は極めて絶望的であるが,之等の患者をよく観察していると,その過高熱の現われ方.その現われる症状等は必ずしも一様ではない。との事は,之等の発熱が一様に温熱中枢からの発熱であつてもその温熱中枢の働き方が必ずしも一様でない事を示していると考えねばならない。
周知の如く,Ranson等によると温熱中枢には熱放散中枢と熱産生中枢の二つが仮定されている。而も熱放散中枢は視床下部のずつと前の部分,即ちPreoptic regionに,熱産生中枢は視床下部の後の部分に存在し,熱放散中枢の方は之を破壊すると熱の放散が妨げられ熱の体内鬱積を来して高熱を来す事になるが,熱産生中枢の方は之を刺戟した時に高熱を起すと云われている。勿論,Ranson等のこの説にも尚幾多疑問の余地が残存している如くであるがう現在の処温熱中枢の所在並びに働き方に関しては最も肯綮に価する説のように考えられている。従つて,この説によると,熱放散並びに産生両中枢が夫々,刺戟された場合,破壊された場合等で現われる症状に差が認められる事は然考えられる。
In this paper, the types and prognosis of the neurogenic hyperthermia occurring shortly after an intracranial operation or a head injury arediscussed on the basis of clinical observations.
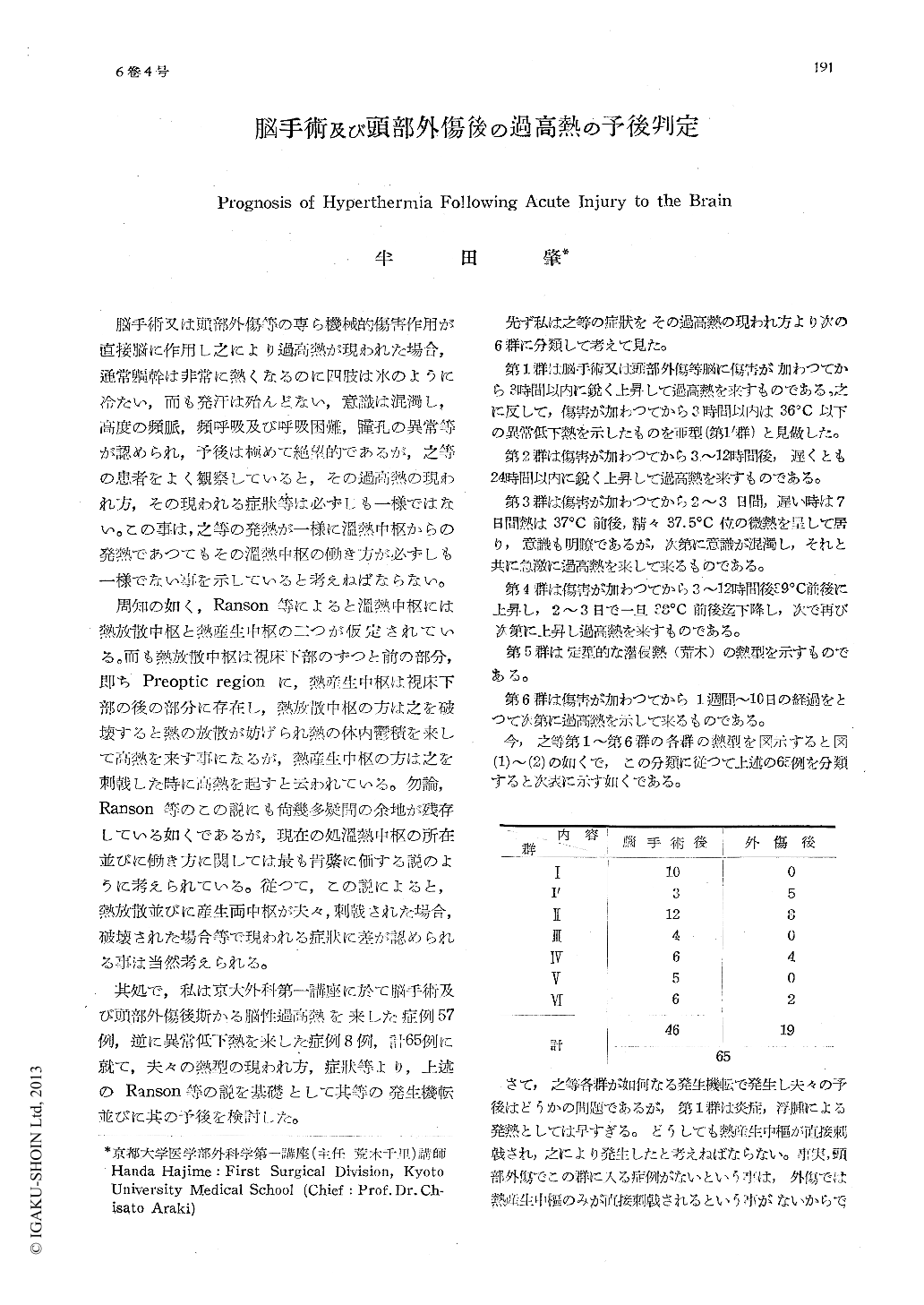
Clinically the following six types of acute neurogenic hyperthermia may be distinguished:
In group (1) hyperthermia is induced within 3 hours following a brain damage. This group is seen only in cases of injuries in or around the hypothalamus and the caudal brainstem.
In group (1') hyperthermia is preceded by the hypothermia lower than 36℃ appearing within 3 hours following an injury and associat-ed with bradycardia and low blood pressure.
In these groups, whatever therapeutic pro-cedures may be undertaken, the fatal outcome is inevitable in 10-15 hours (group (1)) and in 5-10 hours (group (1')).
In group (2) hyperthermia does not com-mence until 3-12 hours, rarely 24 hours after an injury. This seems to be attributed either to brain edema or to absorption of destruction products from the site of the lesion. In this group, some measures such as ice-packs and antipyretic drugs etc. may be occasionally effec-tive, but in most of cases death occurs in the following 15-30 hours.
In group (3) the temperature is maintained between 37° and 37.5℃ during the first 2-3 days, rarely 7 days, but thereafter rises rapidly and reaches over 40℃ accompanied with the disturbance of consciousness. This type seems to the result of postoperative bleeding. In this group, therefore, an emergency operation should be carried out.
In group (4), 3-12 hours after an injury the temperature rises and reaches about 39℃, and within the next 2-3 days the temperature falls transitorily to 38℃ with more or less Perspiration, but thereafter begins to rise again above 40℃. It should be emphasized that in cases of extradural hematoma, where hyper-thermia of this type is not infrequently seen, profuse perspiration is recognized. An emer-gency operation such as exploratory burr holes in the temporal region should be performed.
In group (5), the raised temperature is of the intermittent type, higher in the morning and lower in the afternoon, quite different from the fever in acute surgical infection. This type of hyperthermia was seen in cases of an operation in or around a lateral ventricle, and attributed to the aseptic ependymitis associated with a more or less obstruction of sylvian aqueduct. In this group, therefore, an emer-gency drainage of the lateral ventricle may be advisable.
In group (6) the temperature rises gradually and reaches above 40℃ in the course of 7-10 days and the death ensues. The cause seems to be the hemorrhage within the brainstem.
Copyright © 1954, Igaku-Shoin Ltd. All rights reserved.

