Japanese
English
- 有料閲覧
- Abstract 文献概要
- 1ページ目 Look Inside
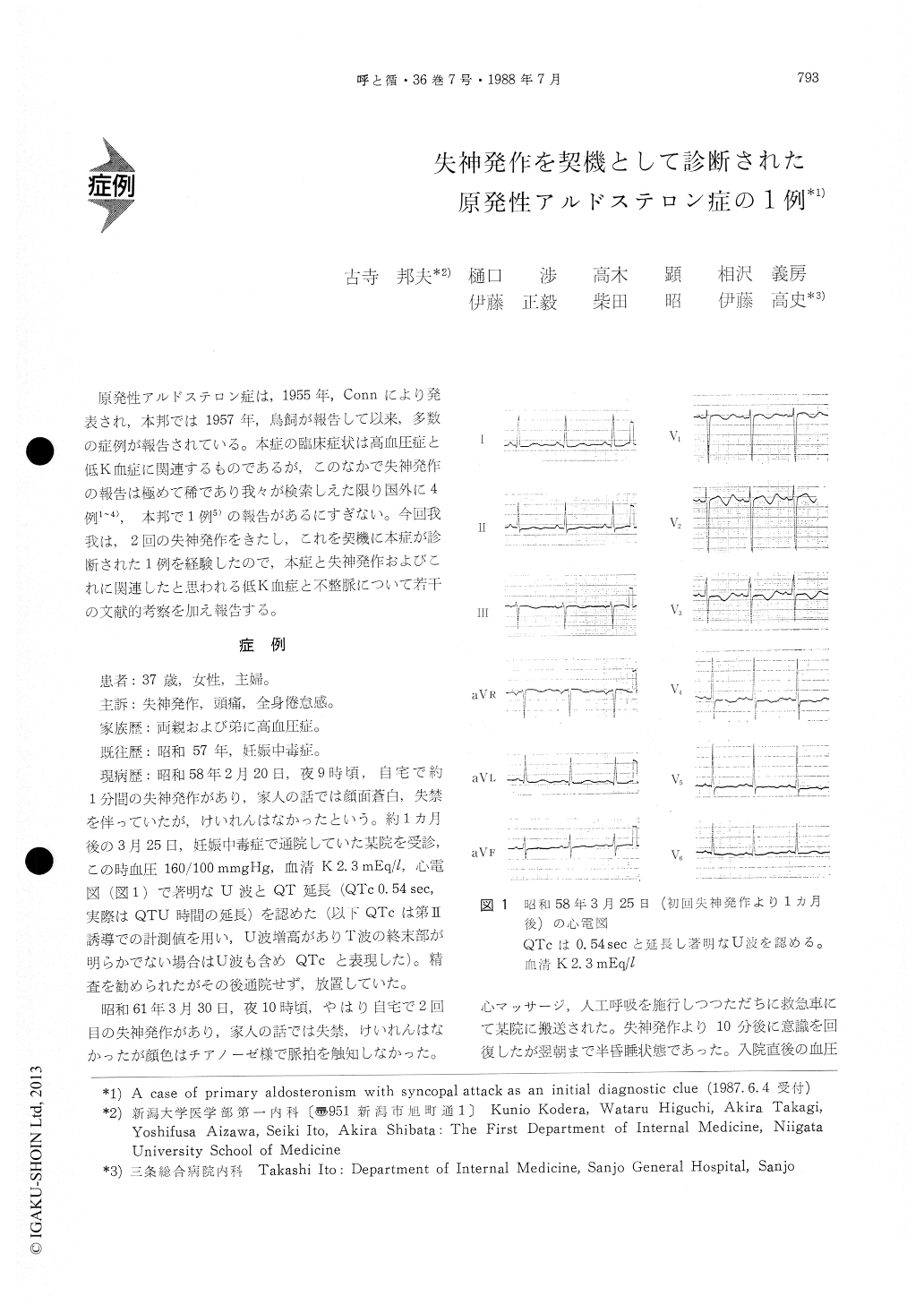
原発性アルドステロン症は,1955年,Connにより発表され,本邦では1957年,鳥飼が報告して以来,多数の症例が報告されている。本症の臨床症状は高血圧症と低K血症に関連するものであるが,このなかで失神発作の報告は極めて稀であり我々が検索しえた限り国外に4例1〜4),本邦で1例5)の報告があるにすぎない。今回我我は,2回の失神発作をきたし,これを契機に本症が診断された1例を経験したので,本症と失神発作およびこれに関連したと思われる低K血症と不整脈について若干の文献的考察を加え報告する。
Syncope is a very rare clinical manifestation of primary aldosteronism. Although primary aldos-teronism is not so rare disease, we know only se-veral reports of such a case. We recently experi-enced a case of 37 years old female, who had two times of syncopal attack during 3 years. After one month from the first syncopal attack, she visited a certain hospital. Then, hypertension (160/100mmHg) and hypopotassemia 3 mEq/liter) were pointed out, but she requested no further examination.
After 3 years from the first attack, she had the second attack in her house. She was admitted to another hospital on ambulance and syncope con-tinued for about 10 minutes. Immediately after the admission, electrocardiogram demonstrated abnor-mal prolongation of QT interval and bigeminal rhy-thm of multifocal ventricular premature complexes and her consciousness was still drowsy. Serum po-tassium concentration was 2. 1 mEq/liter and therefore we supposed that the cause of syncopal attack in this case was attributable to serious ventricular ar-rhythmia, probably ventricular tachycardia or fibril-lation, and that this arrhythmia was induced by severe hypopotassemia.
Her general condition recovered gradually and close examination was undergone about hyperten-sion and hypopotassemia. Hormonal data were strongly suggestive of primary aldosteronism, es-pecially adrenal cortical adenoma, but could not entirely rule out the adrenal hyperplasia. Her sym-ptoms of headache and general fatigue continued.
She was referred to our institute for definite diagnosis after 5 months from syncopal attack. Ele-ctrocardiogram showed typical findnigs of hypo-potassemia, that is, QT prolongation (QTc 0. 54sec), flattening of T wave and prominent U wave. Lo-calization diagnosis was performed by adrenal com-puted tomography, adrenal scintigraphy, and adrenal venous sampling. All results indicated right adrenal cortical adenoma. An operation was performed and adenoma about 15×10×10 mm was resected.
Postoperative course was well. Serum potassium and blood pressure normalized after several days from operation but normalization of QT interval required 5 weeks. Ambulatory electrocardiographic monitoring demonstrated no dangerous arrhythmia.
We stress the clinical importance of syncopal at-tack in primary aldosteronism because syncopal attack becomes sometimes lifethreatening enough.Hypopotassemia and related serious cardiac arrhy-thmia, which may be the cause of synope, should be controlled carefully.
Copyright © 1988, Igaku-Shoin Ltd. All rights reserved.

