Japanese
English
- 有料閲覧
- Abstract 文献概要
- 1ページ目 Look Inside
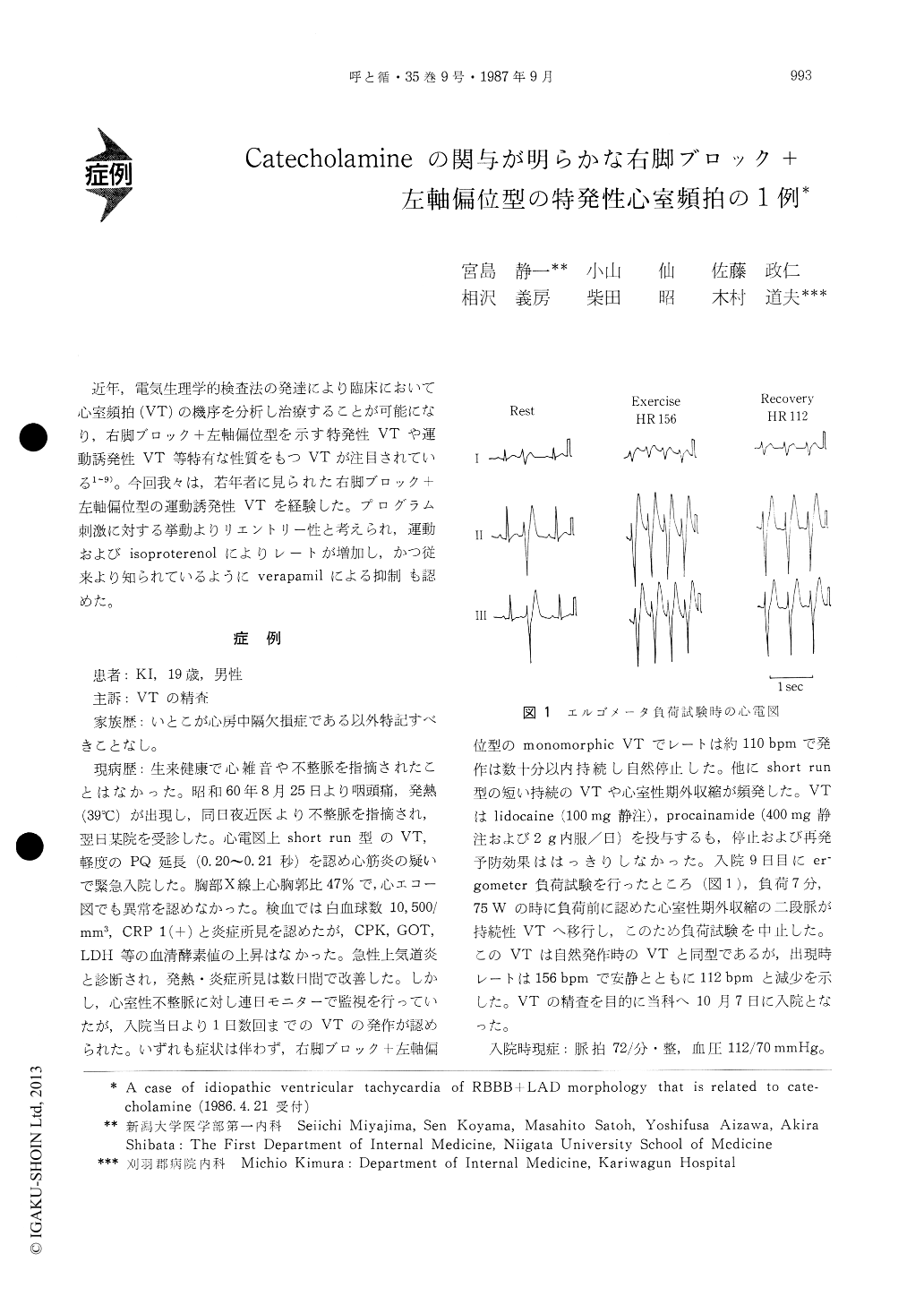
近年,電気生理学的検査法の発達により臨床において心室頻拍(VT)の機序を分析し治療することが可能になり,右脚ブロック+左軸偏位型を示す特発性VTや運動誘発性VT等特有な性質をもつVTが注目されている1〜9)。今回我々は,若年者に見られた右脚ブロック+左軸偏位型の運動誘発性VTを経験した。プログラム刺激に対する挙動よりリエントリー性と考えられ,運動およびisoproterenolによりレートが増加し,かつ従来より知られているようにverapamilによる抑制も認めた。
A 19 year-old-man was admitted to our hospital for further examination of ventricular tachycardia (VT). VT occured several times, but the patient was asymptomatic. The duration of VT was variable and on occasion it sustained. The rate of the VT was 110 bpm and QRS morphology was RBBB+ LAD pattern. VPCs with similar QRS configuration as VT were also observed frequently. During ergometer stress test, bigeminy of VPC of the same QRS morphology as VT progressed to sustained VT with a rate of 156 bpm. After cessation of exercise, the rate of the VT became slower to 112 bpm. Intra-venous lidocaine of 100 mg and 400mg of procainamide could not terminate the VT and oral procainamide of 2 g daily did not prevent the occurence of VT. Then he was admitted to our hospital. Physical status and laboratory examination including echocardio-gram, left ventriculogram and coronary arteriogram showed no abnormality. In electrophysiologic study, ventricular extrastimuli induced nonsustained VT of the same QRS morphology as clinical VT. The rate was 120 bpm. After use of isoproterenol, sus-tained VT with a rate of 170 bpm was reproducibly induced by single extrastimulus given in the right ventricle. The trigger zone was narrow (20 msec). VT was also terminated by extrastimulus. An inverse relationship was obtained between the premature pacing cycle length and the interval from the last paced beat to the first beat of VT. After administration of intravenous verapamil of 10 mg, VT became non-inducible, but when isoproterenol was given, VT was induced by extrastimulus. This time, the rate was reduced to 135 bpm. Several days later, electrophysiologic study was repeated under therapy of oral propranolol of 60 mg daily. Non-sustained VT with the rate of 120 bpm was induced by double extrastimuli from the right ventricle even after addition of intravenous propranolol (4 mg). The mechanism of the VT in this case is considered a reeentry from electrophysiologic study. Slow response fiber may participate in the reentrant circuit, because verapamil slowed the VT rate. Clinically it is important to note the possible situa-tion that the rate of VT can be accerelated by exercise or isoproterenol infusion, which cannot be totally prevented by verapamil.
Copyright © 1987, Igaku-Shoin Ltd. All rights reserved.

