Japanese
English
- 有料閲覧
- Abstract 文献概要
- 1ページ目 Look Inside
後天性冠動脈-心室瘻の報告は非常に稀でそのほとんどが局所的外傷または炎症等により生じたものであり1,2),心筋梗塞後に発生したものは,これまでに3例が報告されているに過ぎない3〜5)。著者らは,陳旧性心筋梗塞の経過中に発生したと考えられる後天性左冠動脈-左室瘻の2例を経験したので報告する。そのうちの1例は,左室瘻出現の前後で冠動脈造影により確認し得た。また,このような冠動脈-左室瘻の形態学的特徴並びに成因について若干の考察を加える。
Acquired coronary artery fistulas after myocardial infarction are extremely rare. We report two cases of left coronary artery fistula opening into the left ventricle which developed during the course of old myocardial infarction. In one of these cases (case 1), serial coronary angiography (CAG) successfully documented the aquired nature of the coronary artery fistula.
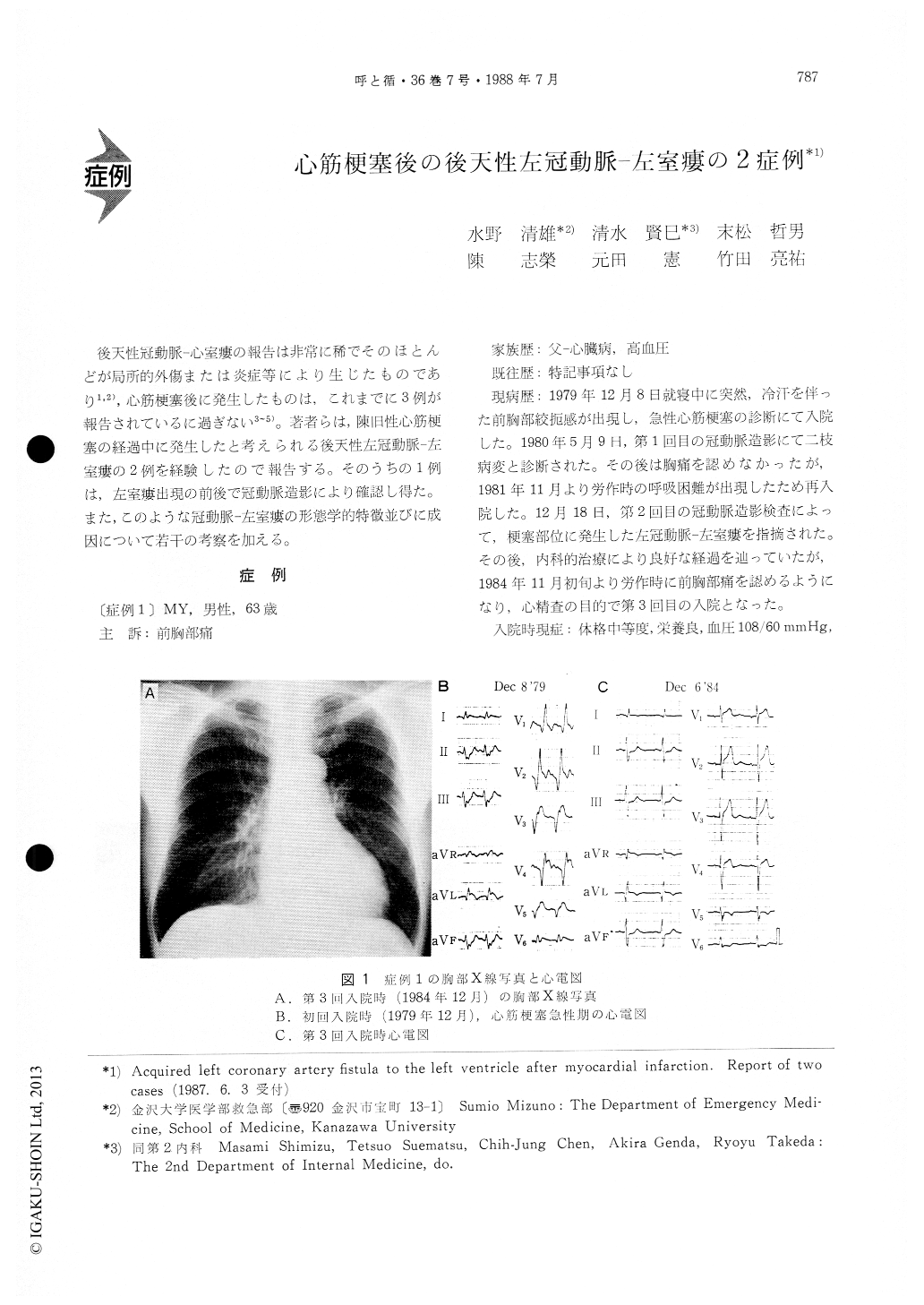
A 63-year-old man (case 1) suffered from severe chest pain with cold sweating and was admitted to our hospital in Dec., 1979. Initial CAG and left ventriculography (LVG) were performed in May,1980. The CAG revealed more than 75% stenosis at the anterior descending (LAD) and circumflex bran-ches of the left coronary artery. The LVG showed reduced motion from the anterior to the posterior wall. In Dec., 1981, repeat CAG and LVG were per-formed because of dyspnea on exertion. There were no changes in the findings of coronary stenosis. However, the CAG showed a fistulous communica-tion between the diagonal and circumflex branches and the left ventricular chamber at the site of the thinned infarcted wall. In Nov., 1984, he was read-mitted, again complaining of chest pain on exertion. The findings of 3rd CAG and LVG showed no par-ticular changes and the fistula had the same profile.
A 55-year-old man (case 2) had a sudden onset of anterior chest pain and was admitted to our hospital in Jan., 1986. After discharge, he noticed mild an-ginal symptoms upon severe exertion and was read-mitted in Dec., 1986. LVG revealed an area of decreased motion of the antero-septal wall and dyskinetic motion in the apex. Selective CAG showed 75% stenosis at the middle portion of the LAD. Furthermore, it was shown that a coronary artery fistula opening into the left ventricular chamber was present at the site of the left ven-tricular apex.
Clinically, these two patients had recurrent chest pain on exertion during the course of old myocardial infarction, but no heart murmur. The characteristics of coronary artery fistula after myocardial infarction are : 1) A small cavity at the site of the thinned infarcted wall. 2) The presence of communicating branches from the coronary artery. Upon CAG, contrast material injected into the coronary artery remains in the coronary artery-ventricular fistula for a while, and then subsequently flows into the left ventricular chamber.
Copyright © 1988, Igaku-Shoin Ltd. All rights reserved.

