Japanese
English
- 有料閲覧
- Abstract 文献概要
- 1ページ目 Look Inside
- サイト内被引用 Cited by
von Recklinghausen病(以下R病と略す)は特有の皮膚病変のほかに,身体のいろいろな部位に多彩な随伴病変を生じる.消化管病変としては,非上皮性腫瘍の合併が知られているが,その報告例は比較的少ない.われわれは,イレウスおよび大量下血で来院した2名のR病患者を手術し,それぞれの小腸に単発性,多発性の神経鞘腫を見出したので報告する.
We report two cases of von Recklinghausen's neurofibromatosis with neurolemmoma of the small intestine.
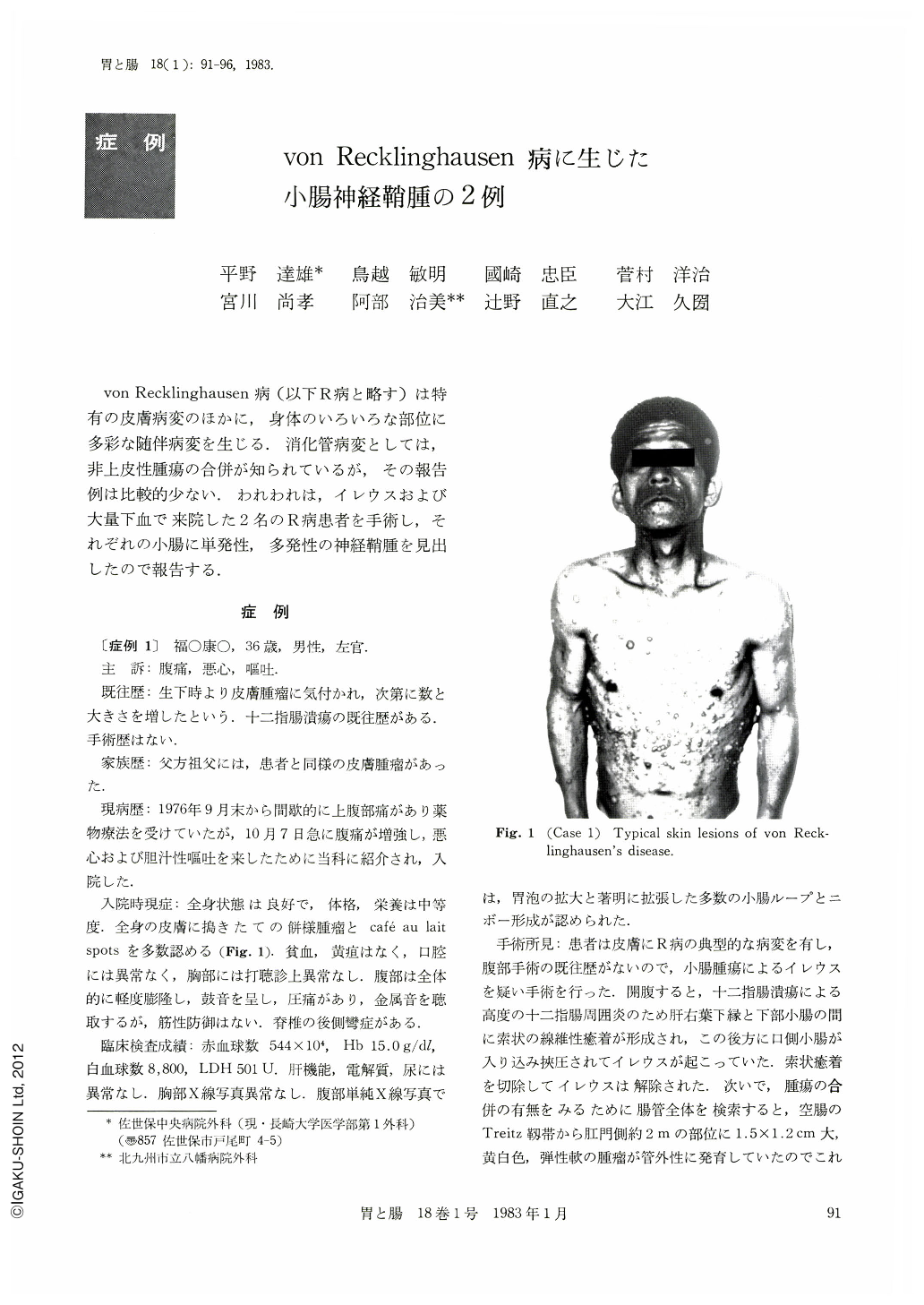
Case 1. A 36-year-old man, in whom von Recklinghausen's disease had been diagnosed previously, was admitted because of upper abdominal pain, nausea and bile vomiting. His paternal grandfather had had similar skin lesions. The past medical history included duodenal ulcer. On physical examination the abdomen was slightly distended, and bowel sound was hyperactive and metalic. Plain abdominal radiogram showed many distended intestinal loops with air-fluid levels. The preoperative diagnosis of intestinal obstruction caused by tumor, especially intussusception, was suspected because he had von Recklinghausen's disease. Although surgical exploration revealed simple intestinal obstruction caused by periduodenal fibrous bands secondary to severe duodenal ulcer, a single serosal neoplasm was detected at the jejunum. Histologically it was neurolemmoma.
Case 2. This 57-year-old woman was admitted in shock because of passing gross blood per rectum. The diagnosis of von Recklinghausen's disease had been made at her age of 50. Her daughter has similar skin lesions, and her son a congenital hydrocephalus. Three days before admission she had passed large bloody stools five times, and her local physician had given intravenous infusion, resulting in the relief of her discomfort. Upon admission the patient appeared pale and apprehensive. Her pulse rate was 120 a minute; the blood pressure 80/60 mmHg. Numerous cutaneous neurofibromas and café au lait spots were noted. The abdomen was not remarkable and rectal examination was negative except that blood was noticed on the examining finger sac. Her hemoglobin was 8.5g%. Neoplasm of the lower small intestine was suspected because of severe hematochezia in von Recklinghausen's disease. After a favorable response to transfusions, she had no further bleeding. Superior mesenteric angiography showed a hypervascular neoplasm at the ileum. Double contrast radiogram of the small intestine demonstrated a niche at the same portion. Surgical exploration revealed one pedunculated tumor extending extraluminally at the distal ileum, and numerous small raised nodules in the serosa of the duodenum and of proximal jejunum. All tumors were removed by segmental resection of the jejunum and ileum and by enucleation of small nodular tumors. Examination of the resected ileum showed ulceration through the mucosa. Histologically the tumors were all neurolemmomas.
In conclusion, as pointed out by Hochberg et al., the possibility of gastrointestinal tumors should be considered in every patient with von Recklinghausen's disease and symptoms of gastrointestinal dysfunction. Since lesions are hypervascular, angiography is thought to be the most helpful in identifying the number and extent of the lesions.
Copyright © 1983, Igaku-Shoin Ltd. All rights reserved.

