Japanese
English
- 有料閲覧
- Abstract 文献概要
- 1ページ目 Look Inside
- 参考文献 Reference
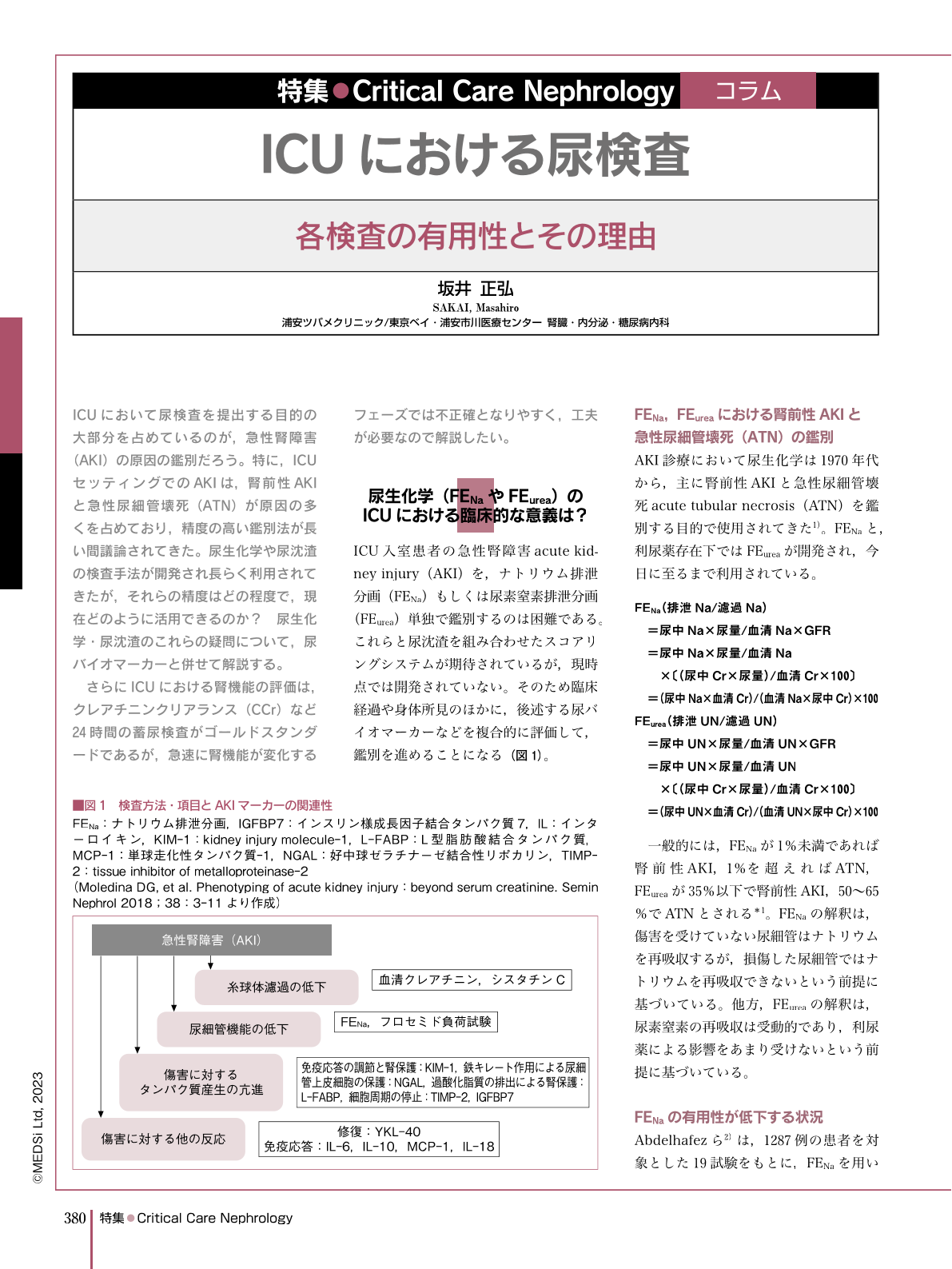
ICUにおいて尿検査を提出する目的の大部分を占めているのが,急性腎障害(AKI)の原因の鑑別だろう。特に,ICUセッティングでのAKIは,腎前性AKIと急性尿細管壊死(ATN)が原因の多くを占めており,精度の高い鑑別法が長い間議論されてきた。尿生化学や尿沈渣の検査手法が開発され長らく利用されてきたが,それらの精度はどの程度で,現在どのように活用できるのか? 尿生化学・尿沈渣のこれらの疑問について,尿バイオマーカーと併せて解説する。
さらにICUにおける腎機能の評価は,クレアチニンクリアランス(CCr)など24時間の蓄尿検査がゴールドスタンダードであるが,急速に腎機能が変化するフェーズでは不正確となりやすく,工夫が必要なので解説したい。
A major reason for performing a urinalysis in the intensive-care unit (ICU) is to determine the causes of acute kidney injury (AKI). In particular, prerenal AKI and acute tubular necrosis (ATN) are the most common causes of AKI in the ICU setting, and their differentiation has long been a matter of debate. Although urinary biochemistry and urinary sediment testing methods have been developed and used for a long time, their accuracy and utility in the current era remain unclear. This article describes findings regarding urinary biochemistry and urinary sediment as well as urinary biomarkers. Furthermore, the gold standard for evaluating the renal function in the ICU is a 24-h urine collection test, such as a creatinine clearance (CCr) assay; however, such tests can be inaccurate in phases with rapid changes in the renal function, so we will discuss how to address this issue.
Copyright © 2023, MEDICAL SCIENCES INTERNATIONAL, LTD. All rights reserved.

