Japanese
English
- 有料閲覧
- Abstract 文献概要
- 1ページ目 Look Inside
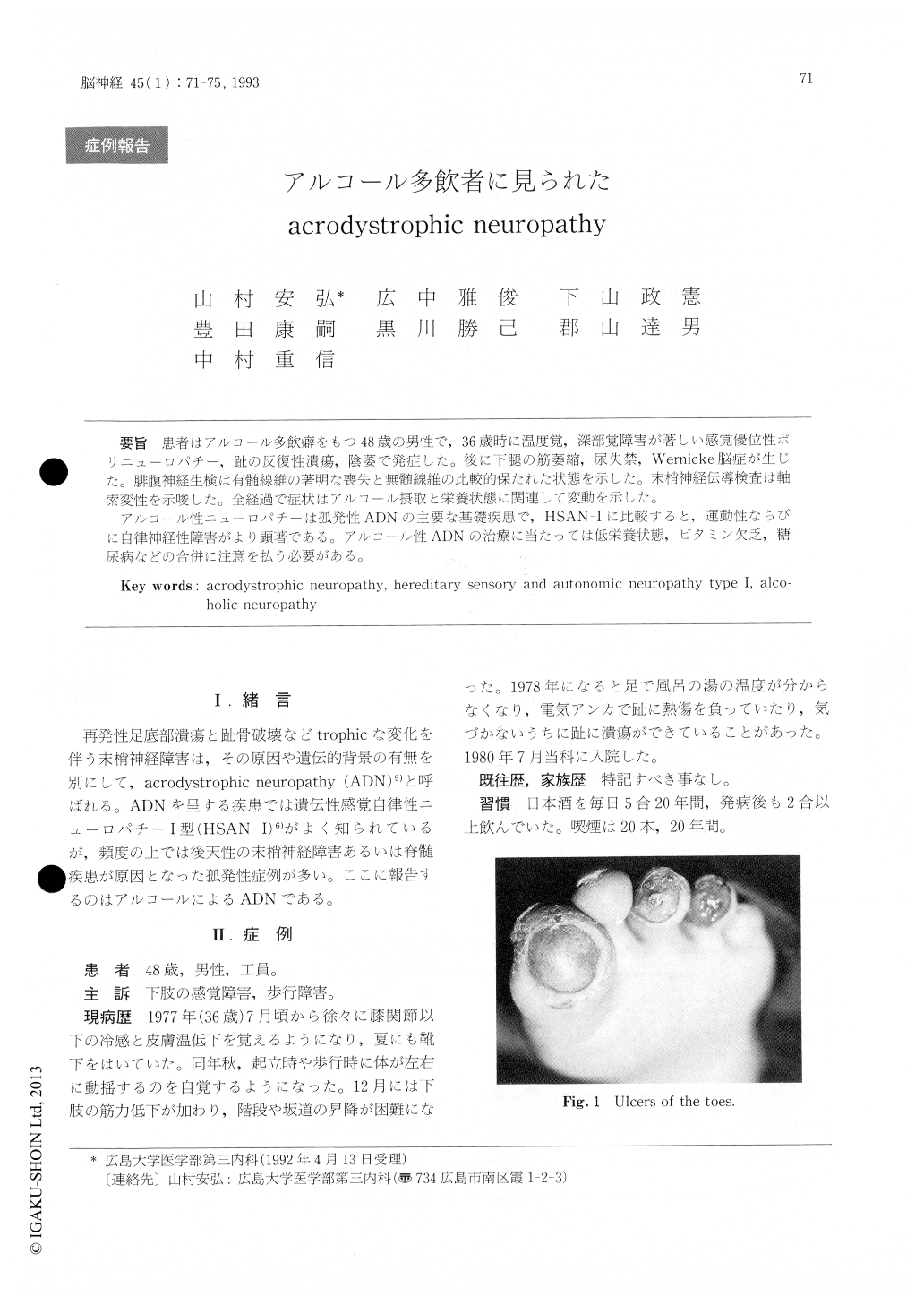
患者はアルコール多飲癖をもつ48歳の男性で,36歳時に温度覚,深部覚障害が著しい感覚優位性ポリニューロパチー,趾の反復性潰瘍,陰萎で発症した。後に下腿の筋萎縮,尿失禁,Wernicke脳症が生じた。腓腹神経生検は有髄線維の著明な喪失と無髄線維の比較的保たれた状態を示した。末梢神経伝導検査は軸索変性を示唆した。全経過で症状はアルコール摂取と栄養状態に関連して変動を示した。
アルコール性ニューロパチーは孤発性ADNの主要な基礎疾患で,HSAN-Iに比較すると,運動性ならびに自律伸経性障害がより顕著である。アルコール性ADNの治療に当たっては低栄養状態,ビタミン欠乏,糖尿病などの合併に注意を払う必要がある。
The patient was a 48-year-old alcoholic man with no contributory family history. At age 36 he had developed sensory dominant polyneuropathy with highly impaired temperature sensation and deep sensation in the lower extremities, recurrent ulcers of the toes, and sexual impotence. A sural nerve biopsy at this time revealed marked loss of myelinated fibers with relative preservation of the population of unmyelinated fibers. Subsequently, he developed muscle atrophy of the lower thighs, uri-nary incontinence, and Wernicke's encephalopathy, and became non-ambulatory at age 44. The periphe-ral nerve conduction findings suggested predomi-nantly axonal degeneration. The entire course was characterized by alternative progression and partial recovery influenced by his alcohol intake and nutri-tional state.
Alcoholic neuropathy is a major cause of solitary acrodystrophic neuropathy (ADN). Manifestations of autonomic and motor neuropathy are more marked in alcoholic ADN than in HSAN-I, and central nervous system involvement is the hallmark of alcoholic ADN. In the treatment of patients with alcoholic ADN, attention should be paid to diabetes mellitus, malnutritional state, and vitamin deficiency, which frequently complicate alcoholism.
Copyright © 1993, Igaku-Shoin Ltd. All rights reserved.

