Japanese
English
- 有料閲覧
- Abstract 文献概要
- 1ページ目 Look Inside
I.はじめに
若年性一側上肢筋萎縮症は平山,豊倉,椿により1959年6)にはじめて報告され,1963年7),1972年8)に追加記述される一方,国内各地での報告もあいつぎ,外国からの報告1,15,17)はまだ少ないが,Clinical Entityとしてほぼ確立したと考えられている。これまでの臨床観察から,この一群の患者の示す特徴点が明確にされたが,その病因については不明のままである。従来から本症は,髄節性障害が強調されてきた8,13,16,18,19)が,最近,広瀬ら9)は腕神経叢障害の可能性を指摘した。これまでわれわれは,本症の障害筋分布に注目して,筋電図検査を行つてきたが,今回26例について筋電図学的に本症の病態を検討したので,病変部位の検討を含め,臨床的に指摘されている本症の諸特徴との対比を行つた。
In 1959, this disorder was first reported by one of authors (K. H.) (6). Scince then, many Japanese cases have been reported and recently some cases are also reported in other countries. Its cause and pathology are still unknown, because no autopsy case was obtained. In this report, some electro-myographic findings are described and discussed.
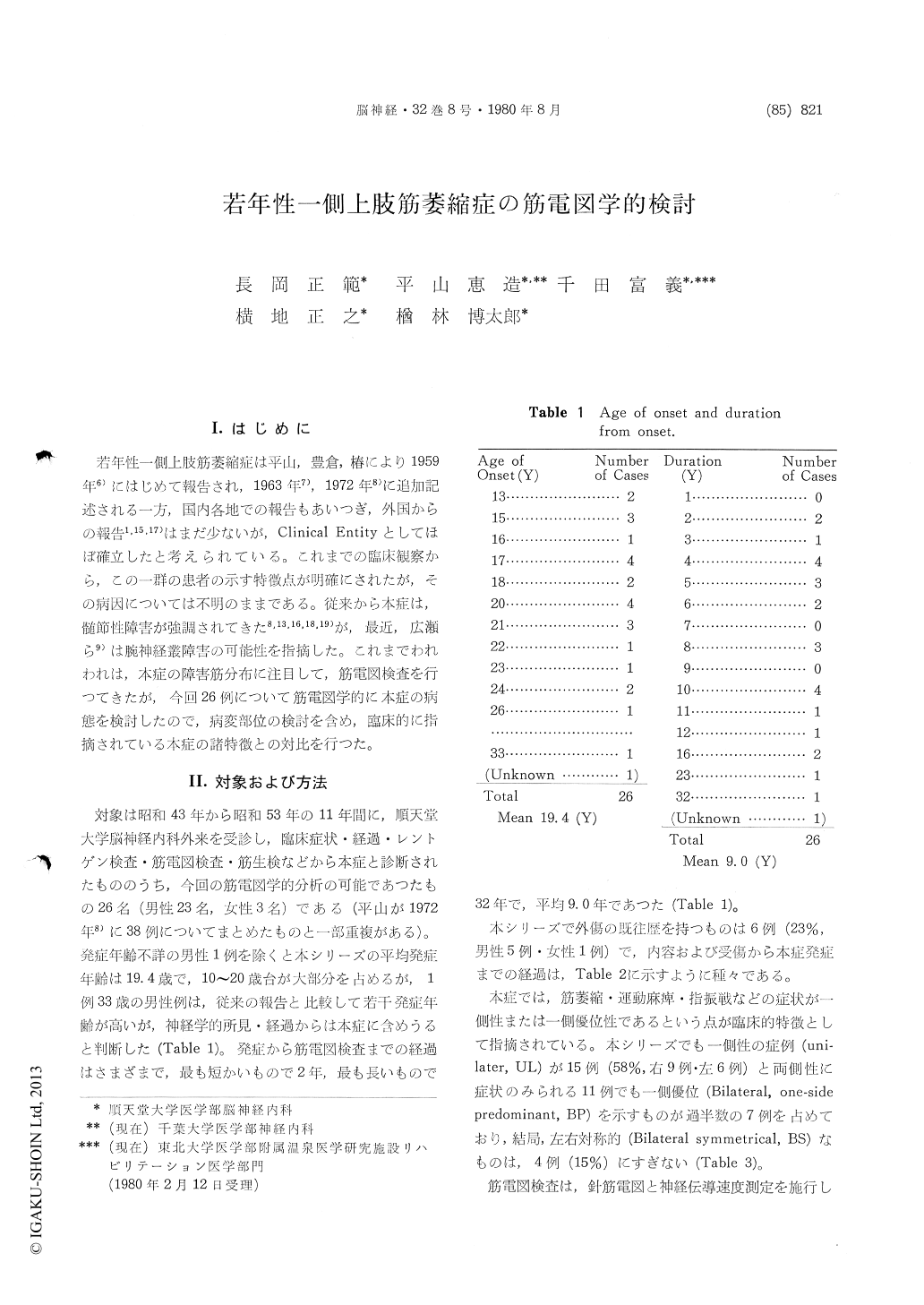
This series contain 26 cases (male 23, female 3). Age of onset: 13-33 years old (mean 19.4 years old). Clinical duration: 2-32 years (mean 9.0 years). Only 6 cases (23%) showed trauma as the past history (Table 2). We classified 26 cases in three groups (UL: unilateral, BP: bilateral, one-side predominant, BS: bilateral symmetrical) based onthe laterality of physical findings (amyotrophy, weakness, finger tremor, etc.) (Table 3).
Conventional needle EMG were done in all cases and these findings were judged by the criteria which we defined as Fig. 2. In some cases, con-duction velocity (MCV & SCV) were measured.
Needle EMG showed more selective and localized distribution of NGP (neurogenic pattern) in the hand muscles, the forearm muscles except for M. brachioradialis, and M. triceps brachii on the atro-phied sides of the arm in all clinical groups (UL, BP, BS) (Table 4・5). On the normal side of bi-laterally examined cases of UL group, NGP was shown in 9/11 cases, but its distribution seemed to be slightly restricted in the more distal part. Thus, in this disorder, 22/26 cases (77%) were electromyo-graphically affected on the bilateral sides, although the clinical feature was mostly unilateral. The clinical features and pathological process seemed to be estabilished in a few years after the onset with-out the apparent tendency of further progression. Afterwards, no apparent extension of NGP distri-bution and increment of grading were observed in the clinical course. No delay was observed on MCV and SCV.
The pathological lesions responsible for these electromyographic changes are discussed, either on spinal segmental origin or on brachial plexus ori-gin, but some ambiguous portions are still re-mained.
Copyright © 1980, Igaku-Shoin Ltd. All rights reserved.

