Japanese
English
- 有料閲覧
- Abstract 文献概要
- 1ページ目 Look Inside
I.はじめに
小児の間脳下垂体疾患では小人症,尿崩症,錐体路症状をみることは稀ではない。また器質性の下垂体性小人症はしばしば中枢性尿崩症を伴う。一方では,小人症—網膜色素変性—皮膚病変—知能障害を示すCockayne症候群1,2)や小人症—網膜変性—皮膚病変—知能障害—錐体路症状を示すSjögren-Larsson症候群は,その多彩な症状で名高いが病因として確実にあげられるものはない。
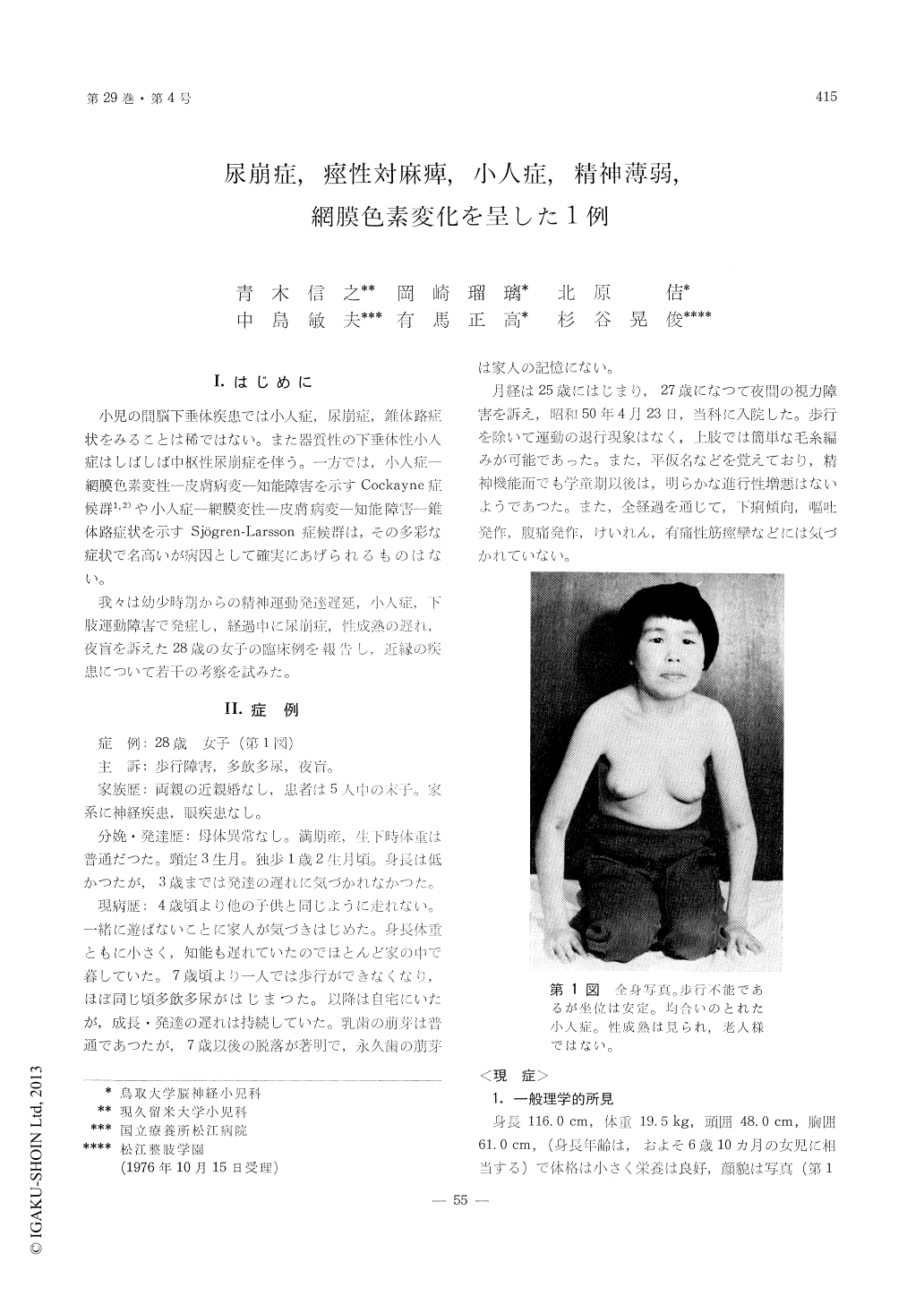
我々は幼少時期からの精神運動発達遅延,小人症,下肢運動障害で発症し,経過中に尿崩症,性成熟の遅れ,夜盲を訴えた28歳の女子の臨床例を報告し,近縁の疾患について若千の考察を試みた。
A 28-year-old, mentally retarded female was ad-mitted to the hospital with the complaints of stunted growth, polyuria, and night-blindness. She was a product of nonconsanguinous marriage and normal pregnancy. She had 4 elder siblings, and no patient with neurological or ophthalnic disease was present in her family. She was born with normal birth weight without abnormalities in her neonatal period. In infancy her growth and development appeared normal and walked at 14 months of age. At the age of 4 years, she was noted to fall down easily and her growth and mental development appeared to be delayed. Gait disturbance progressed. She became unable to walk without support at the age of 7 years when polydipsia and polyuria began. The teeth tended to become worn down in child-hood, and adontia persisted thereafter. At 25 years of age, menarch began. At the age of 27, she be-gan to complain night-blindness. Convulsion, vomiting, diarrhea or severe abdominal pain had not been experienced.
On admission, small statue (116.0 cm height, 19.5 kg weight), microcephalus (48.0 cm), mental retard-ation (IQ 57) and motoric disturbance were noted.Physical and neurological examinations revealed adontia, spastic paresis of the lower extremities with Babinski sign and clonus, mild cataract, squint, optic atrophy and retinitis pigmentosa of the pepper and salt type. Other cranial nerves, cerebellar and vestibular functions, speech, hearing, and sensory systems appeared normal. Skin, hair, chest, ab-domen, nails, dermatoglyphix, and other structures were not particular.
On laboratory examinations, polyuria with a low specific gravity was constantly noted. It was cor-rected by the injection of pitressin. Endocrinolo-gical examinations showed a dysfuction of the hypothalamus-pituitrary system with a low urinary 17 OHCS and 17 KS excretion, low GH and T4 levels, and a poor response to arginine. Rentgeno-logical examinations including carotid angiography and pneumoencephalography did not show any finding suggesting tumor. Chromosome analysis, determinations of serum electrolytes, immunoglo-bulins, GOT, GPT, urea N, Ca, P, lipid fraction, lactate, pyruvate, and uric acid, urinary amino acids, motor conduction velocities, and the serological tests for syphilis showed all normal results. He-matological examinations were normal except for mild hypochromic anemia. No lymphocytic vacu-oles were observed.
The symptom-complex as observed in this patient was compared with those of other known syndromes accompanied by dwarfism and retinar degeneration. The multiple manifestations involving the pyramidal tracts, mental function, hypothalamo-pituitary sys-tem, retina, and lens in the present patient appear to originate from a common metabolic abnormality.
Copyright © 1977, Igaku-Shoin Ltd. All rights reserved.

