Japanese
English
- 有料閲覧
- Abstract 文献概要
- 1ページ目 Look Inside
I.はじめに
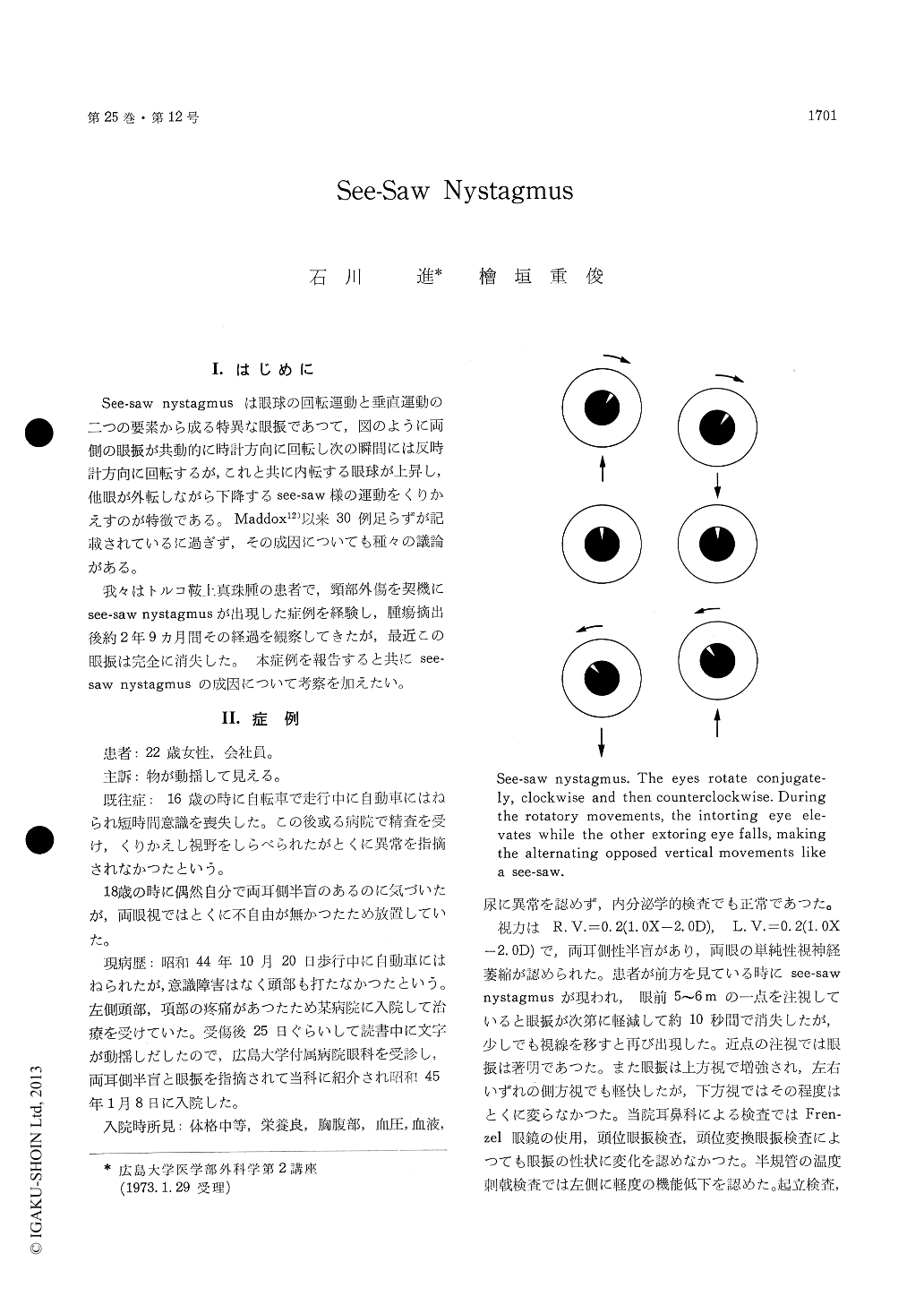
See-saw nystagrnusは眼球の回転運動と垂直運動の二つの要素から成る特異な眼振であつて,図のように両側の眼振が共動的に時計方向に回転し次の瞬間には反時計方向に回転するが,これと共に内転する眼球が上昇し,他眼が外転しながら下降するsee-saw様の運動をくりかえすのが特徴である。Maddox12)以来30例足らずが記載されているに過ぎず,その成因についても種々の議論がある。
我々はトルコ鞍上真珠腫の患者で,頸部外傷を契機にsee-saw nystagmusが出現した症例を経験し,腫瘍摘出後約2年9カ月間その経過を観察してきたが,最近この眼振は完全に消失した。 本症例を報告すると共にsee—saw nystagmusの成因について考察を加えたい。
See-saw nystagmus is a peculiar type of dis-sociated rotatory-vertical nystagmus in which the eyes rotate conjugately clockwise and then counter-clockwise. In addition to the rotatory movements, the intorting eye elevates while the opposite ex-torting eye falls, making the alternating opposed vertical movements like a see-saw. Since the des-cription of the original case of see-saw nystagmus (Maddox, 1913), less than 30 cases have been re-ported. Pathophysiology of this rare condition is controversial and several sites, such as ocular sys-tem, brain stem, diencephalon, combined lesions or multiple levels, have been suggested to produce this nystagmus.
We have had the opportunity to study an inter-esting patient. A 22-year-old woman was admitted to our department on January 8, 1970, having noted oscillopsia following cervical injury. Four years prior to admission she recognized a bitem-poral hemianopsia by herself. However, she had not consulted a physician because of lack of any other trouble.
General physical and hormonal examination was normal. Visual acuity was 0.2 in each eye but corrected to 1.0 by concave lens. Mild bilateral optic atrophy and a typical bitemporal hemianopsia were demonstrated. A classical see-saw nystagmus was apparent in all directions of gaze and most marked in upward gaze. The nystagmus was diminished on distant gaze and became marked on near gaze.
Caloric stimulation revealed a slight imbalance between the two vestibular systems. The second and the third cervical vertebrae were tender on percussion and the bilateral greater occipital nerves were painful on compression.
Neuroradiological examinations revealed a large suprasellar mass lesion. Right frontal craniotomy was performed and a suprasellar epidermoid tumor was encountered. Cheesy material was removed and portions of the thin capsule were excised. Macroscopic diagnosis was confirmed by histological examination.
Following surgery the nystagmus became in-conspicuous for several days but returned to the preoperative state. The nystagmus was diminished with either eye patched and also relieved in supine position on the patient. Cervical sympathetic block with 8 to 10 cc of Xylocaine inhibited tem-porarily the nystagmus. This procedure probably gave the effect on the both of the anterior and the posterior sympathetic systems. Cervical sympathetic block was repeated and CDP-choline, which activates the brain stem reticular formation, was administered. The nystagmus became grad-ually inconspicuous, and then disappeared com-pletely 2 years and 8 months after the surgery.Aat that time visual fields recovered to almost normal.
In this patient multiple factors, such as dience-phalic, ocular and cervical, seem to play each role in causing the see-saw nystagmus. As suggested by Ishijima, Sekino et al., a see-saw nystagmus may be produced by a disturbance of a delicatebalance in the supranuclear mechanisms controlling ocular movements in the brain stem, where various inputs from the cerebrum, the vestibular system, the cerebellum and the neck are integrated by a complicated multisynaptis network and output signals are sent to the ocular motor nuclei.
Copyright © 1973, Igaku-Shoin Ltd. All rights reserved.

