Japanese
English
- 有料閲覧
- Abstract 文献概要
- 1ページ目 Look Inside
はじめに
第三脳室後半以下の閉塞が疑われる症例の診断に,Monro孔経由,第三脳室内にカテーテルを滑りこませ,空気または陽性造影剤を注入するcentral ventriculo—graphyがよく用いられるが,挿入カテーテルの位置の判定に毎常image intensifierが利用できるとは限らず,カテーテルを介して術者の手指に伝わる抵抗をたよりに挿入が行なわれることも多い。かかるとき,一応,適当と思われる深さにまでカテーテルを挿入し,その確認のため,単純撮影を行なうと,カテーテルの先端は第三脳室底を穿破してchiasmatic cisternに達していたり,側脳室底を後方に滑走し,時にはquadrigeminal ciseternに至っていたりして,冷汗三斗の思いをすることもまれではない。またたとえimage intesifierを用いるとしても,Monro孔の位置を知ることは不可能で,あまりに突飛な方向へのカテーテルの滑りを防止するに役立つにすぎない。
われわれはこのような盲目的挿入を避けるため内視鏡の利用を考え,Monro孔を直接観察下において,安全確実なカテーテルの挿入を行なうとともに,Monro孔を含む側脳室壁,さらに極めて細い内視鏡を第三脳室内へと挿入して,第三脳室壁の血行動態の観察や,腫瘍その他の病的異物の有無,その性状などの観察記録を試みてきた。いまだ症例が充分でなく,装置そのものにも今後改良すべき点が多く,あくまでもpreliminary reportに止まるが,最近第三脳室腫瘍として,短絡手術,次いでCo深部照線を行ない,長期間経過を観察するも,症状の改善が得られなかった一症例に対し,内視鏡検査を行なったところ,腫瘤がMonro孔を経て側脳室内へと膨出しているのが観察され,その所見より剔除可能な嚢腫と想定されたため直接手術に踏み切り,手拳大のまれな奇形腫の企剔に成功,術後諸症状の著明な寛解を得ることが出来たので,ここに症例の報告をかね,内視鏡で現在までに得られた成績の若干を紹介する。
This is a report of a case in which huge teratoma in the third ventricle (76 gm) was completely ex-triated. In this case, endoscopic examination per-formed prior to the operative procedure, gave re-liable information regarding the pathology of the tumor and a surgical exposure of the third ventricle was indicated.
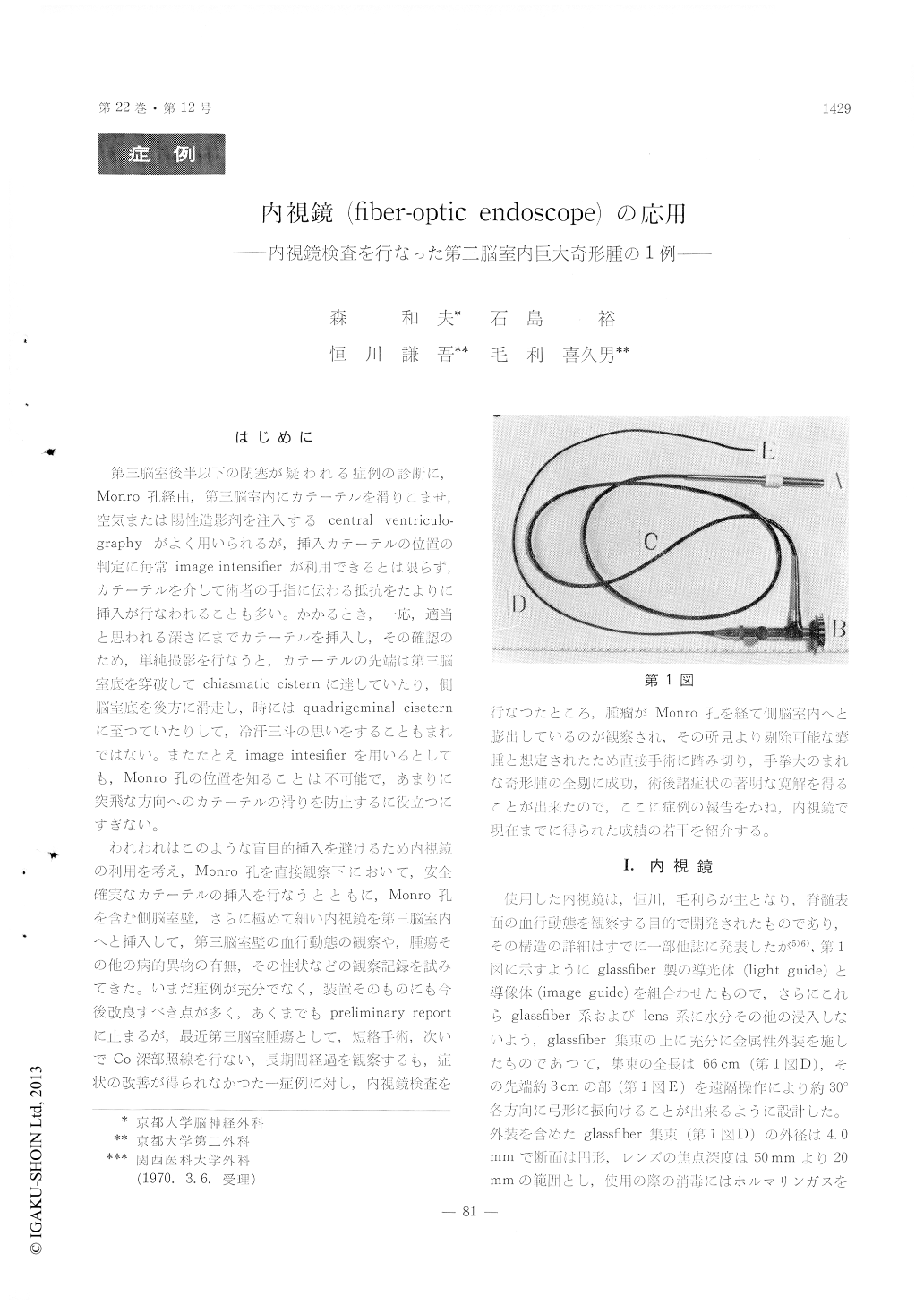
A fiber-optic endoscope : The newly designed in-strument, as shown in Fig. 1, is consisted of a glas-sfiber image- as well as light-guide and waterproffed by metal coating. The glassfiber assembly has an outer diamiter of about 4. 0 mm, enough to smallto pass through the foramen of Monro. Further-more, a flexible tip of this assembly, (E in Fig. 1), enables us, to some extents, to turn the instrument to any desired direction. We have succeeded to insert this instrument into the third ventricle with-out any diffculties to observe small vessels of the tela chorioidea. Fig. 2 illustrates a Nelaton's catheter which has been introduced into th foramen of Monro with safe and accuracy under the endoscopic direct visualization of the foramen.
Case report : 4 year boy was admitted to our clinic with a state of akinetic mutism, bilateral papilledema and positive Parinaud' sign. Ventriculography re-vealed the presence of a large mass located in the third ventricle (Fig. 3). Following the decompres-sive procedure (ventriculo-peritoneal shunt opera-tion), 60Co radiotheraphy was done which, hewever, proved not to be effective. Moreover, occasional attacks of parkinosonian tremor and rigidity as well as coarse athetoid movements of the upper limbs were also observed during the periods of conservative theraphy
Endoscopic examination applied prior to the opera-tion, revealed that a smooth milk-white tumor of a ginko nut size peeped into the right lateral ventricle through the foramen of Monro (Fig. 4). By observ-ing its apparance, it was assumed that the tumor was cystic and could be attacked radically.
A craniotomy was performed with total extripa-tion of the tumor which was sharply demarcated by conective tissue capsul and could be readily dis-sected away from adjacent structures. The extri-pated tumor measured 4 × 4 × 7. 5 cm, in size and 76 gm in weight with multilobular cystic cavities. Histologically, it was classified as a teratom consist-ing tridermal elements. No mitoses or area of in-vasion were found (Fig. 6 and 7).
After the operation, patient was aleviated from a state of akinetic mutism as well as coarse extra-pyramidal hyperkinesia. He returned to an infant school and has been well for about 1 year.
Our newly designed endoscope would offer many advantages in the neurosurgical field to find out the presence of a pathology deep in the brain. Especially it is of potential value for making accurate diagno-sis of a mass located in the third ventricle, because there are no reliable methods available for deter-mining (from clinical examination or ventriculo-graphy) which existed tumor is malignant and which is bengin.
Copyright © 1970, Igaku-Shoin Ltd. All rights reserved.

