Japanese
English
- 有料閲覧
- Abstract 文献概要
- 1ページ目 Look Inside
定型的Wolff-Parkinson-White (WPW)症候群の心電図ではPQ時間の短縮とΔ波が特徴的所見とされる。しかし,標準12誘導心電図では,心室早期興奮が明らかでない例もあり,臨床上その診断は必ずしも容易ではない。
今回我々は副伝導路を介する順行性房室伝導が遅い,いわゆるslow Kentのため,定型的WPW症候群の心電図所見を呈さず,運動負荷心電図を含めて診断が難しくadenosine-5-triphosphate (ATP)静注が診断上極めて有用であったWPW症候群の1例を経験したので報告する。
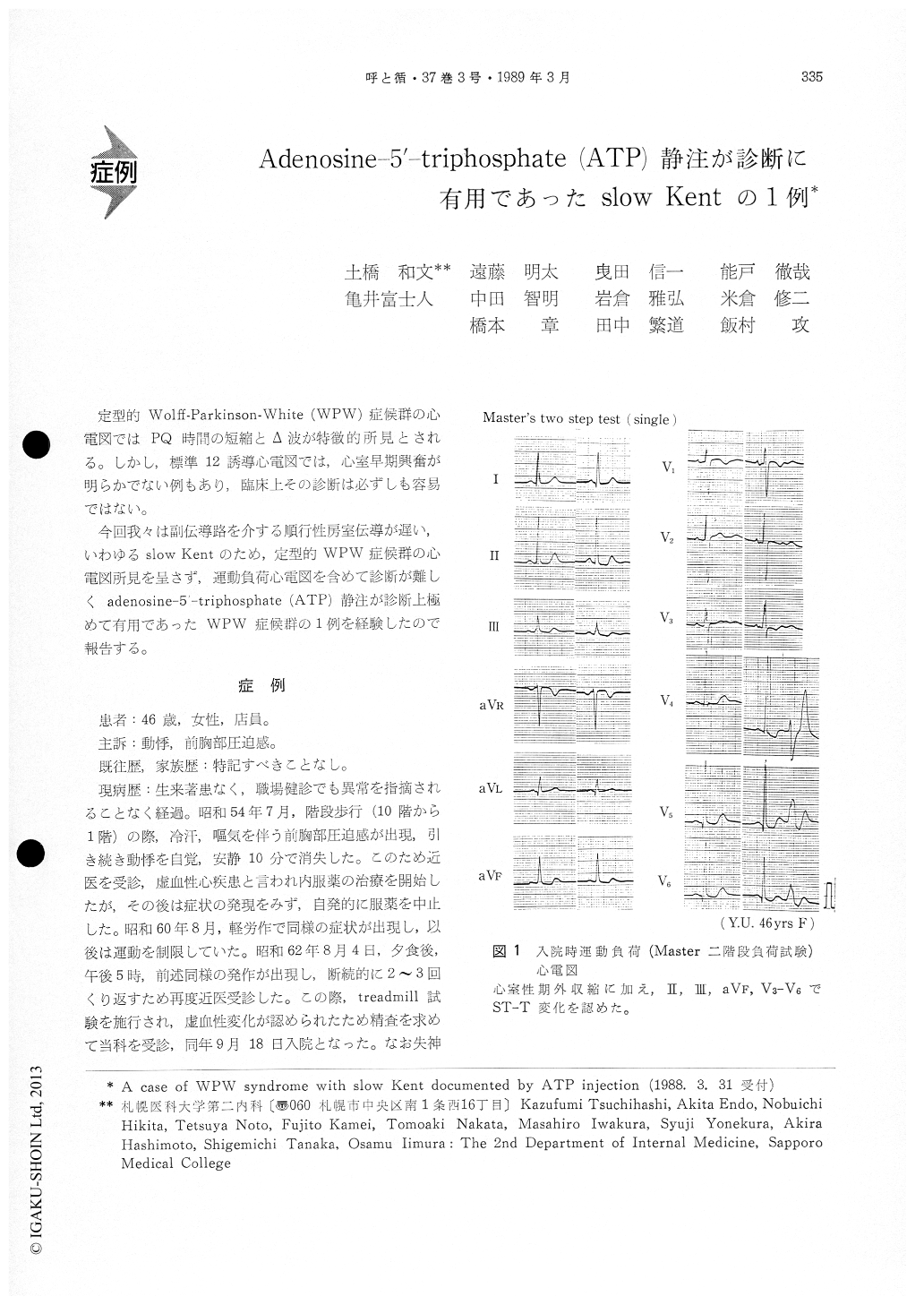
A 46-year-old woman with chest tightness and palpitation at exercise was admitted to Sapporo Me-dical College Hospital for the evaluation of the ST-T changes on stress electrocardiogram. In this patient, PQ time was 0.14 second and pre-exitation was not clearly documented on electrocardiogram at rest.
Bolus injection of 10 mg of adenosine-5'-triphos-phate (ATP) demonstrated deltawave through theelongation of antegrade conduction of atrio-ventri-cular (AV) node. Electrophysiological study also showed left lateral accessory pathway with slow antegrade conduction, slow Kent. Stress 201-Tl myocardial scintigraphy using bicycle ergometer did not show the existence of ischemic region in spite of the ST-T changes on electrocardiogram. In this case, it seemed that a false positive ST-T changes might be caused by ventricular pre-exitation through slow Kent fiber.
From these findings, it was suggested that the transient interruption on conduction through AV node by ATP bolus injection may be an useful di-agnostic method in borderline pre-exitation syn-drome.
Copyright © 1989, Igaku-Shoin Ltd. All rights reserved.

