Japanese
English
- 有料閲覧
- Abstract 文献概要
- 1ページ目 Look Inside
完全房室ブロックに拡張期房室弁逆流が認めらねることは,すでに指摘されている所であるが1,2),特に方法面の制約から,同血流の病態生理学的意義に関する検討は未だ充分なされていない。近年,超音波パルスドプラ法の登場3〜5)で心内血流動態が比較的容易に把握可能となり,各種心疾患に伴う異常血流動態の検討も数多くなされるようになってきており,同法の病態評価に対する有用性が高まってきている6,7)。今回著者らは,超音波パルスドプラ法を用いることにより,完全房室ブロック例における拡張期房室弁逆流の有無を検討し,その特微を明らかにするとともに,同血流に伴う左室内異常血流動態について分析し,拡張期僧帽弁逆流の病態生理学的意義について考察を試みたので報告する。
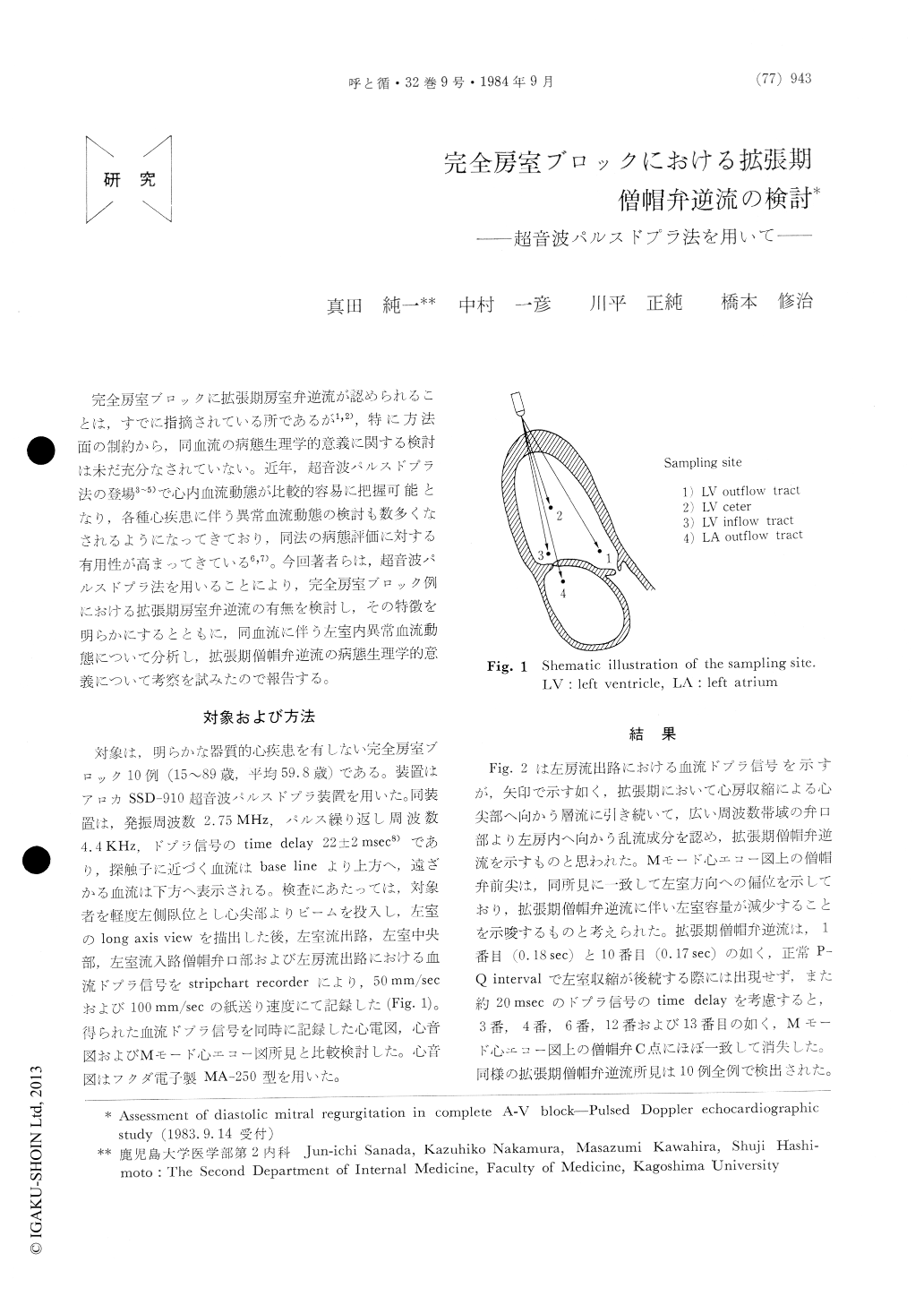
In order to visualize the patho-physiological significance of diastolic mitral regurgitation in the cases with complete A-V block, 10 cases with complete A-V block and without apparent organic heart diseases were studied using pulsed Doppler echocardiography. All of them showed disturbed mitral regurgitant flow at the left atrial outflow tract, immediately after the laminar flow caused by left atrial contraction. Mitral regurgitant flow disap-peared at the C-point of M-mode echocardiogram suggesting that mitral valve closure was completed by left ventricular isovolumic contraction. Thus, isovolumic contraction flow, that occurred simul-taneously with the strain of chorda tendinea and the change of left ventricular shape, and made a revolution in the left ventricular cavity, was believed to contribute to mitral valve closure mechanism.
On the other hand, in the 3 of 10 cases, it appeared that the longer the preceding P-Q interval, the shorter the Q-IIA interval and the duration of left ventricular ejection flow. Moreover, in one of these 3 cases, apparent II-sound splitting was observed at the cardiac cycle in which IIA occurred earlier. In the other 2 cases, II-sound splitting was obscure because early occurrence of IIP was shown in the same manner as IIA. These observations were inter-preted to indicate the fact that diastolic mitral regurgitation was one of the cause of early occur-rence of IIA, and may result in II-sound splitting in the cases with complete A-V block.
Copyright © 1984, Igaku-Shoin Ltd. All rights reserved.

