Japanese
English
- 有料閲覧
- Abstract 文献概要
- 1ページ目 Look Inside
ここ十年あまり本邦における胃疾患診断の進歩はめざましく,胃隆起性病変についても数多くの珍しい症例の発表がなされてきた.
著者らは,浮腫と低蛋白血症を主訴として来院し,胃ポリーポージスによる蛋白漏出性胃症と考えられた症例を経験したので報告したい.
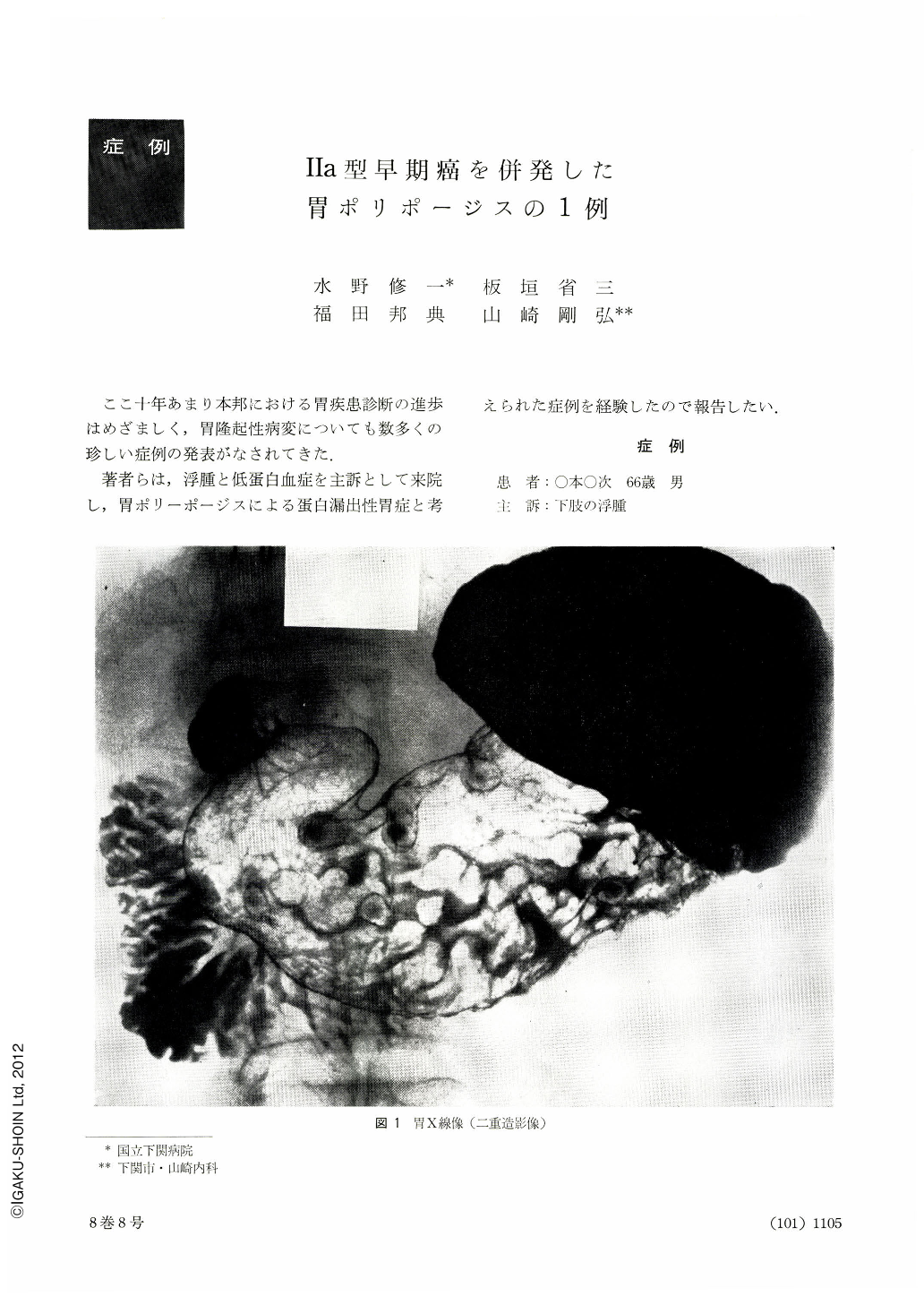
Diagnostic workup of a 66-year-old man, hospitalized on account of edema in the lower extremities, revealed gastric polyposis associated with hypoproteinemia and minor degree anemia. Scores of polyps studded the gastric mucosa over the areas of the corpus and antrum. Gastrectomy was performed as it was apparent that the polyps had given rise to protein-losing gastropathy. Both the small intestine and colon were free from them.
Gross observation of the resected stomach showed about 30 polyps scattered about over both walls of the corpus and antrum. Mostly they were solitary, but partly two or three polyps fused into one. Most of them had slight central dips, histrogically erosions, at the tip. All the polyps belonged to the type Ⅱ as classified by Nakamura. It was presumed that repeated episodes of gastritic inflammation had resulted in the formation of polyposis. In addition, a broad-based plateau-like elevation, 20 mm in diameter, was seen in the antrum. Histologically it proved to be Ⅱa type adenocarcinoma tubulare with sm degree of depth invasion. We assume that reiteration of inflammation played a part in bringing about cancer development.
Differentiation from Ménétrier's disease must be taken into account, but we are of the opinion that gastric polyposis should not be included in this disease. Absence of intestinal polyposis, subcutaneous nodular tumor, and of pigmentation of the skin and mucosa precludes the possibility of Gardner's or Peutz-Jegher's syndrome.
Copyright © 1973, Igaku-Shoin Ltd. All rights reserved.

