Japanese
English
- 有料閲覧
- Abstract 文献概要
- 1ページ目 Look Inside
胃Reactive Lymphoreticular Hyperplasia(以下R. L. H.と略称)は,臨床的に,胃癌との鑑別診断が困難である.
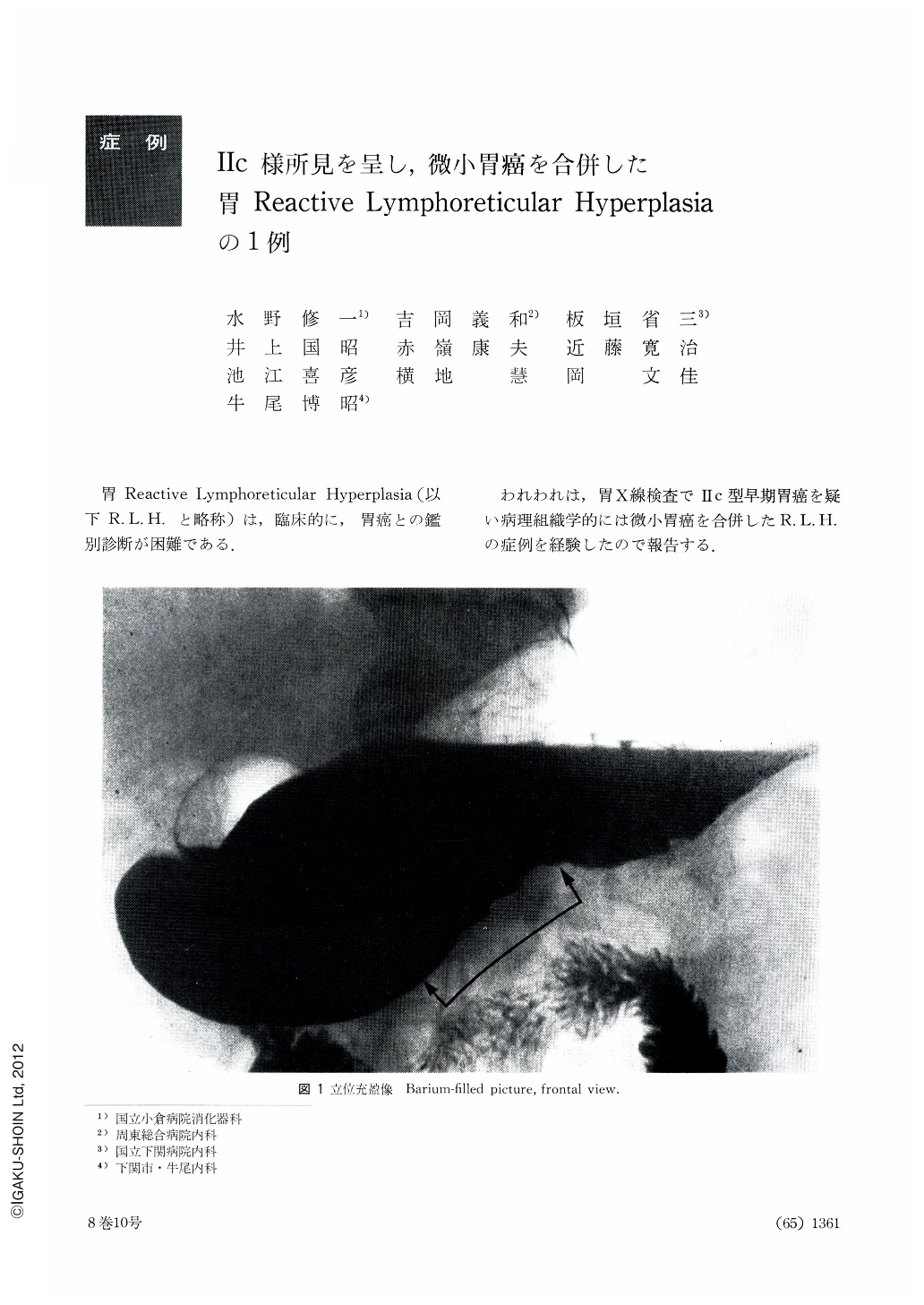
われわれは,胃X線検査でⅡc型早期胃癌を疑い病理組織学的には微小胃癌を合併したR. L. H.の症例を経験したので報告する.
A 53-year-old man was admitted to the hospital for thorough workup because of epigastric pain and feeling of abdominal distension. The status praesens at admission was non-contributory expect slightly high blood pressure. Laboratory examinations were all within normal limits. X-ray and endoscopy of the stomach revealed a depressed lesion in the mucosal folds, which were gigantic. Biopsy failed to reveal any malignancy, but the patient underwent gastrectomy under a strong suspicion of a IIc subtype early cancer. Histologic examination of the excised specimen disclosed that reactive lymphoreticular hyperplasia (RLH) accounted for the parts of hypertrophy and depression on the mucosal folds. At the same time we found IIc subtype early cancer, 9 by 7 mm, on the posterior wall in the border region between the fundic and pyloric gland areas. The early cancer was surrounded with a strip of lymphocytic infiltration. The depth of invasion was sm, and histologically the lesion was differentiated tubular adenocarcinoma.
Gastric RLH so closely resembles early cancer of the stomach excepting type I not only in the findings of x-ray and endoscopy but in those of gross observation that accurate distinction between them depends on the results of cytologic diagnosis or biopsy. When local erosion or ulcer is associated with RLH, it is usually intractable and the patient often suffers from persistent complaints. Differentiation from individual early cancer cases is not always easy, so the RLH thus found is considered at the present moment as an indication for surgical removal. It remains to be seen, however, whether RLH of the stomach left untouched would undergo malignant changes in the future.
Copyright © 1973, Igaku-Shoin Ltd. All rights reserved.

