Japanese
English
- 有料閲覧
- Abstract 文献概要
- 1ページ目 Look Inside
- 参考文献 Reference
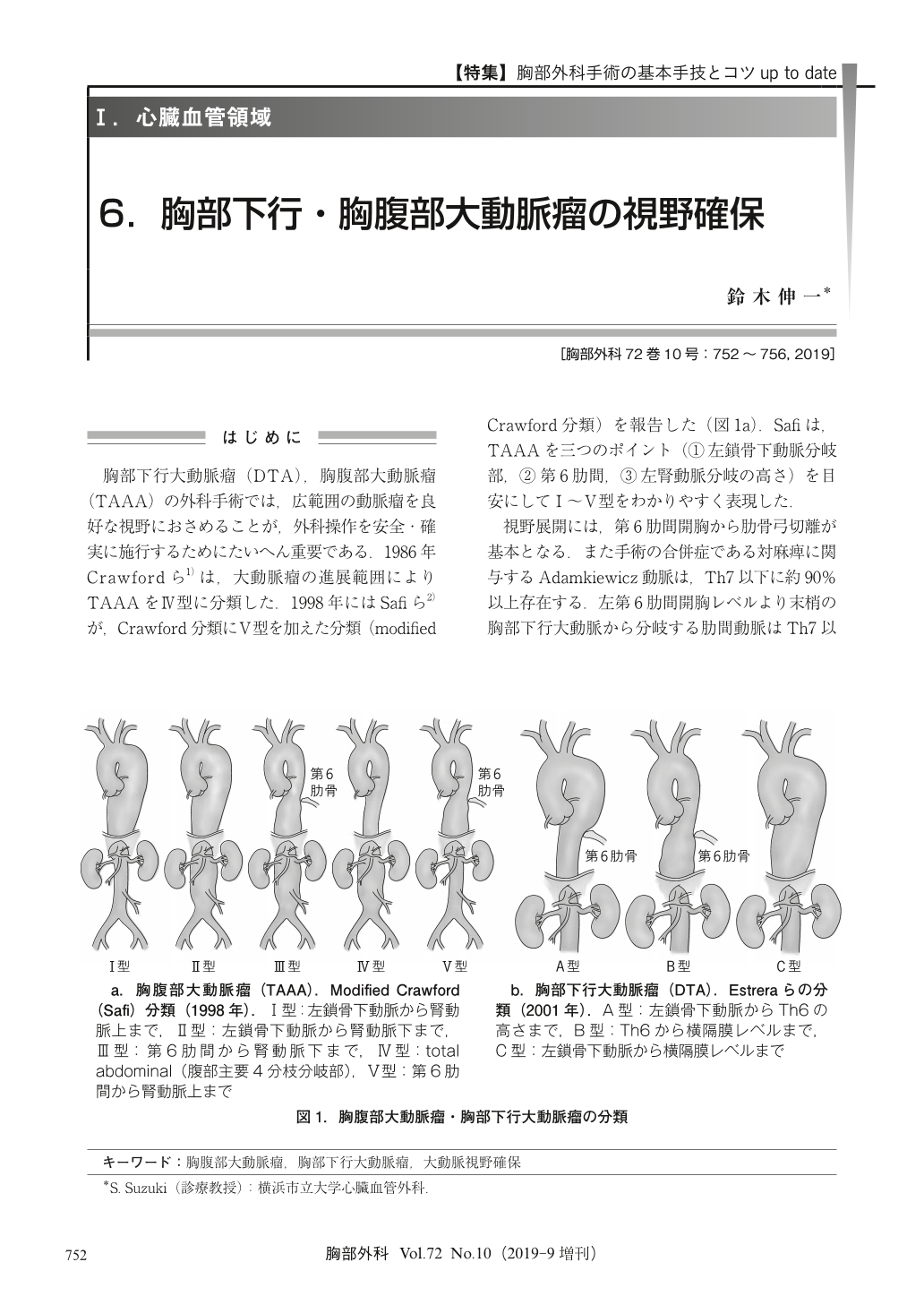
胸部下行大動脈瘤(DTA),胸腹部大動脈瘤(TAAA)の外科手術では,広範囲の動脈瘤を良好な視野におさめることが,外科操作を安全・確実に施行するためにたいへん重要である.1986年Crawfordら1)は,大動脈瘤の進展範囲によりTAAAをⅣ型に分類した.1998年にはSafiら2)が,Crawford分類にⅤ型を加えた分類(modified Crawford分類)を報告した(図1a).Safiは,TAAAを三つのポイント(①左鎖骨下動脈分岐部,②第6肋間,③左腎動脈分岐の高さ)を目安にしてⅠ~Ⅴ型をわかりやすく表現した.
Good exposure of aortic lesions is very important to perform the surgery for descending thoracic aneurysm (DTA) and thoracoabdominal aortic aneurysm (TAAA). The patient is positioned in the right lateral decubitus position with the shoulders at 90°, and the hips flexed to 45°. A left thoracoabdominal skin incision is made in the 6th intercostal space beginning at the posterior axillary fold, and is extended through the costal cartilage and obliquely across the abdomen. The left chest cavity is exposed through the 6th intercostal space, and the costal arch is divided, then the descending thoracic aorta is exposed. The abdominal aorta is exposed through the retroperitoneal cavity. The dissection of diaphragm is carried out to expose the aortic hiatus. When the diaphragm is cut to get better exposure, it is circumferentially cut, at the muscle edge of approximately 2 cm. Then the aortic lesion of extent Ⅱ TAAA, which is all of thoracoabdominal aorta, can be exposed. Lung and abdominal organs should be retracted gently to avoid the damage of them.
© Nankodo Co., Ltd., 2019