Japanese
English
- 有料閲覧
- Abstract 文献概要
- 1ページ目 Look Inside
- 参考文献 Reference
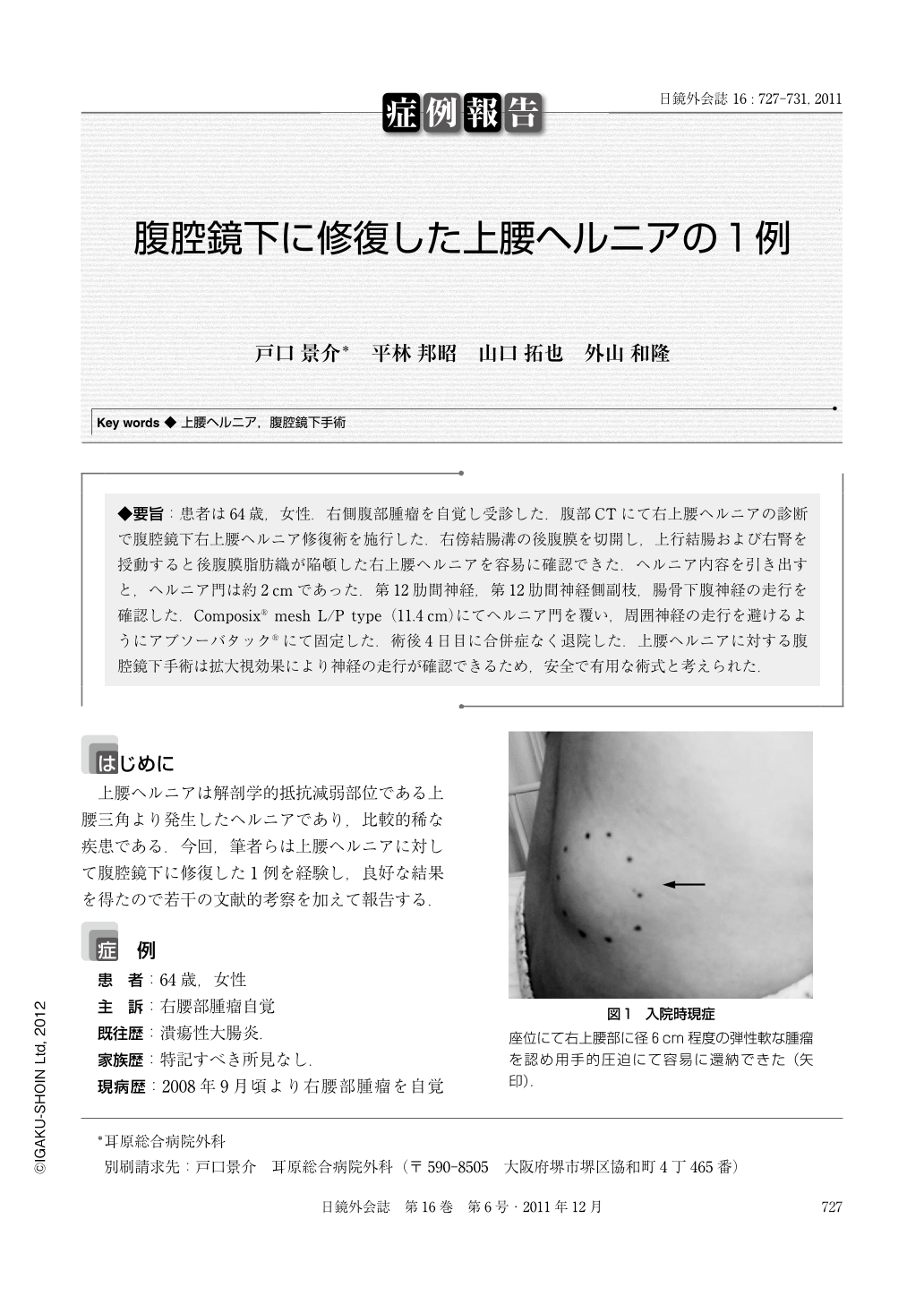
◆要旨:患者は64歳,女性.右側腹部腫瘤を自覚し受診した.腹部CTにて右上腰ヘルニアの診断で腹腔鏡下右上腰ヘルニア修復術を施行した.右傍結腸溝の後腹膜を切開し,上行結腸および右腎を授動すると後腹膜脂肪織が陥頓した右上腰ヘルニアを容易に確認できた.ヘルニア内容を引き出すと,ヘルニア門は約2cmであった.第12肋間神経,第12肋間神経側副枝,腸骨下腹神経の走行を確認した.Composix® mesh L/P type(11.4cm)にてヘルニア門を覆い,周囲神経の走行を避けるようにアブソーバタック®にて固定した.術後4日目に合併症なく退院した.上腰ヘルニアに対する腹腔鏡下手術は拡大視効果により神経の走行が確認できるため,安全で有用な術式と考えられた.
A 64-year-old woman visited our department with a chief complaint of a mass at the right lumbar area. Computed tomography offered a diagnosis of superior lumbar hernia. We repaired her superior lumbar hernia by laparoscopic surgery. We cut the peritoneum of the para colic gutter. After mobilizing the right kidney, the incarcerated fat was visible in the superior lumbrar hernia We pulled out the contents of hernia and hernia gate was about 2cm. We visulized the 12th intercostals nerve, the collateral branch of 12th intercostals nerve and the iliohypogastric nerve. We covered the gate of the superior lumbar hernia by a composix mesh L/P type (11.4cm)® and fixed the mesh by absorba tack® .We avoided the surrounding nerve when we fixed the mesh. She was discharged from the hospital on the forth post operative day without complication. We considered that laparoscopic surgery for superior lumbar hernia was a safe and effective technique because we could visualize the nerves which were magnified by laparoscopy.
Copyright © 2011, JAPAN SOCIETY FOR ENDOSCOPIC SURGERY All rights reserved.

