Japanese
English
- 有料閲覧
- Abstract 文献概要
- 1ページ目 Look Inside
I.はじめに
髄膜癌腫症Meningeal Carcinomatosis(以下MC)は,1870年のEberthの報告3)に始まり,最近の脳腫瘍全国統計では転移性脳腫瘍の5.5%を占めるとされている24).一般に多彩な臨床症状や高度の頭蓋内圧亢進等を呈し,急速に進行,予後不良な重篤な疾患群として知られている.これまで多くの臨床病理学的報告10,12,13,22)があるが,最近は早期診断や治療法の工により生存期間の延長も報告されている11,17,18,21).しかしながら本病態の頭蓋内圧分析による報告はきわめて少なく,経過中に出現する頭蓋内圧亢進の様相は単に漠然と理解されているにすぎない.今回われわれは,MCの頭蓋内環境を解明する一助として持続頭蓋内圧測定を行い,その圧分析の検討を中心に臨床的考察を行ったので報告する.
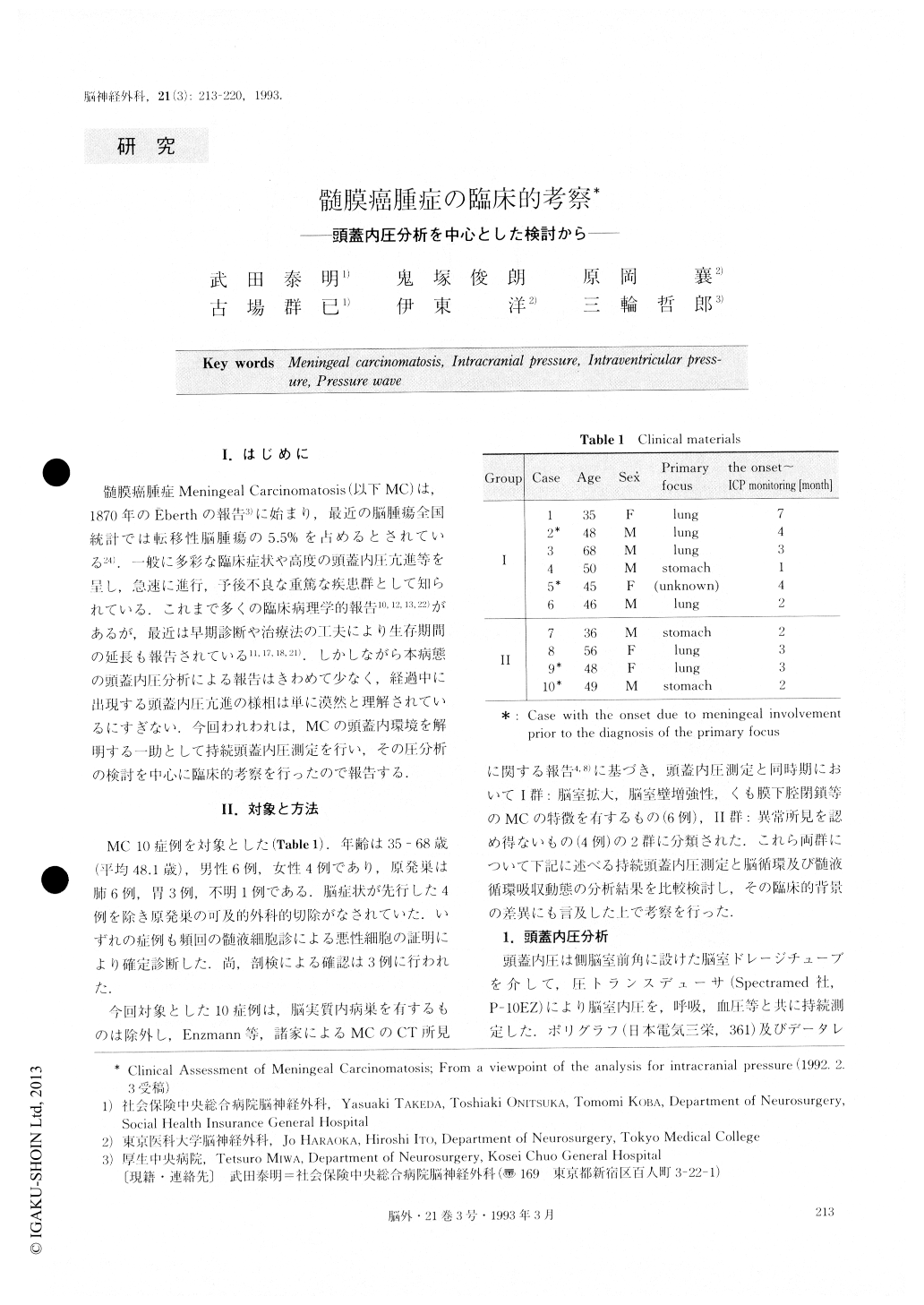
Meningeal carcinomatoses (MC) have been mainly studied from the viewpoint of the analysis of intracra-nial pressure (ICP). From the CT findings, ten patients were divided into two groups: group I, six patients showed characteristics of MC; group II, four showed normal characteristics. Ventricular fluid pressure (VFP) was continuously measured by a controlled ventricular drainage tube using a Spectramecl P-10EZ at 3.1 ± 2.1 months after the onset of the neurological symptoms.At the same time as VFP monitoring, the CBF by 1“3Xe method was measured in 5 cases and RI cisternography was performed in 9 cases.
”A“ wave was observed in 5 cases of group I and in 3 cases of group II. ”B“ wave was observed in all cases of both groups. In all 10 cases, the occurrence rate of both A and B waves (ORA, ORB) were high, averaging 2.34±0.54 times/hour, 74.0±16.6% time, respectively. Mean resting pressure(R) and mean peak pressure(P) tended to be high, averaging 28.8±12.2mmHg, 58.9 13.7mmHg, respectively. Mean cerebral perfusion pres-sure corresponding with R and P (CPPR, CPPp) was markedly reduced, averaging 79.1±15.9mmHg, 50.9± 12.7mmHg, respectively. Both ORA and ORB in group Iwere higher, and both CPPR and CPPp in groupl were lower, than in group II. Statistically, this is significant. Both R and P in Group I tended to be higher than in group II. This has no statistical significance. CBF in all 5 cases averaged 34.8±8.4mI/100g/min. No significant difference in the impairment of CBF was found between both groups. RI cisternography showed delayed clearance in all 9 cases. This was espe-cially evident in group I.
As to the clinical aspects, the neurological symptoms appeared earlier, and were more various in group I than in group II. In contrast to these, concerning the marked increase of CSF-protein content, the degree of ventricu-lar dilatation on CT scan, and the clinical outcome, the difference between both groups was scarcely signifi-cant.
In conclusion, MC is presumed to be ”tight brain" characterized by the elevation of resting pressure, the frequent occurrence of pressure wave, and the reduc-tion of cerebral perfusion pressure. Great care is de-manded for accurate diagnosis of MC, and the need for treatment is urgent. This is so because whether or not CT scan discloses pathognomonic findings it is not at all uncommon that MC has already developed to a condition with disorder of CBF and CSF flow dyna-mics. Additionally, the degree of the progression on CT findings does not always parallel the change of im-paired ICP and CBF. Furthermore, the pathophysiolo-gy of MC must be analyzed more minutely, and ther-apeutic guidelines based on multilateral evaluation methods remain to be established in the future.
Copyright © 1993, Igaku-Shoin Ltd. All rights reserved.

