Japanese
English
- 有料閲覧
- Abstract 文献概要
- 1ページ目 Look Inside
I.はじめに
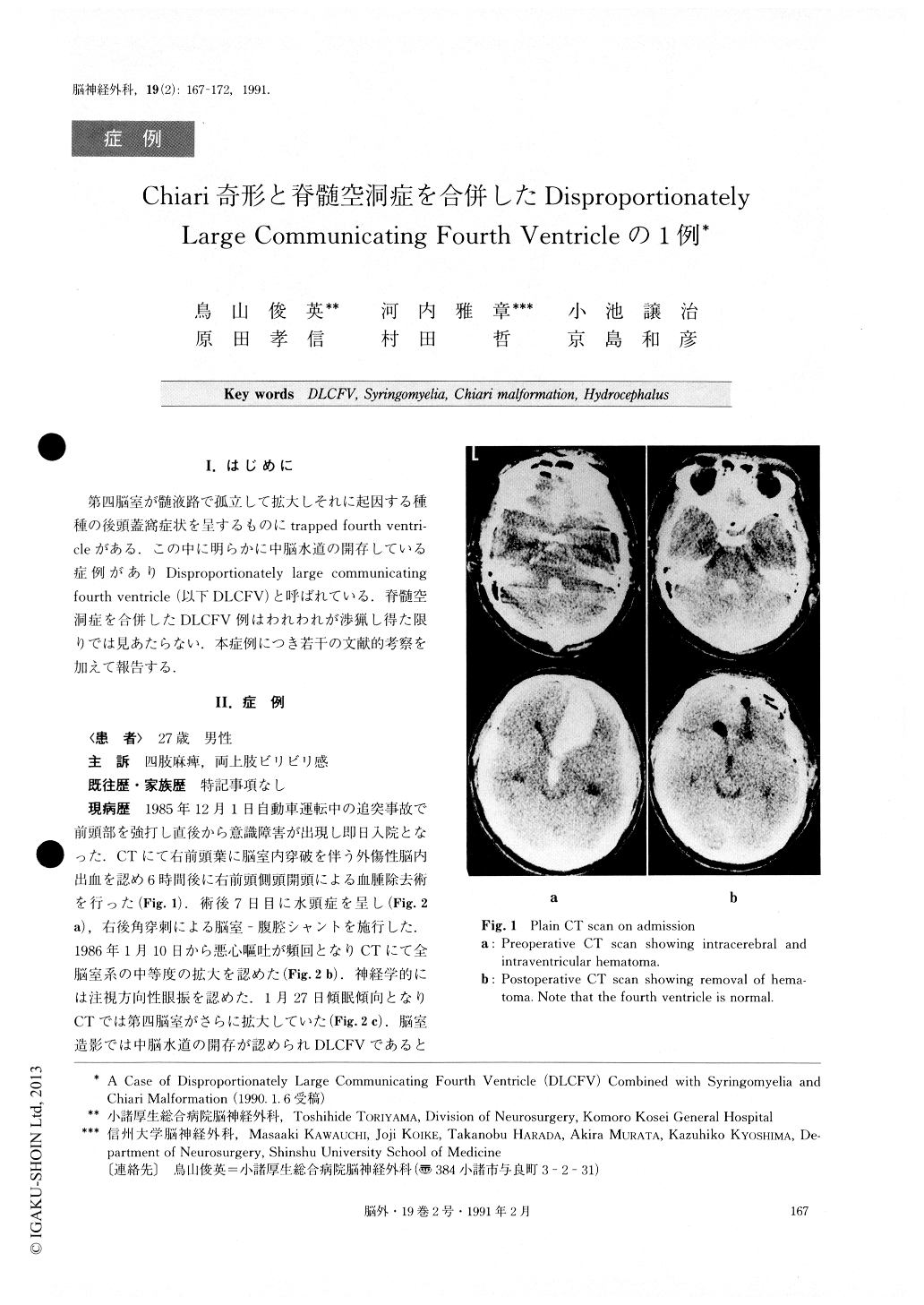
第四脳室が髄液路で孤立して拡大しそれに起因する種種の後頭蓋窩症状を星するものにtrapped fourth ventri—cleがある.この中に明らかに中脳水道の開存している症例がありDisproportionately large communicating fourth ventricle(以下DLCFV)と呼ばれている.脊髄空洞症を合併したDLCFV例はわれわれが渉猟し得た限りでは見あたらない.本症例につき若干の文献的考察を加えて報告する.
Abstract
We report a rare case of disproportionately large communicating fourth ventricle (DLCFV) combined with syringomyelia and Chiari malformation. The case was a 27-year-old male who underwent ventriculoperi-toneal (V - P) shunt on the right side for hydrocepha-lus caused by traumatic intracerebral and intraventricu-lar hemorrhage. One month later, he became somnolent with posterior fossa symptoms (nausea, vomiting and nystagmus). CT scan demonstrated enlarged fourth ventricle, which was diagnosed as DLCFV because the ventriculogram revealed patency of the aqueduct. One and half month later a second V - P shunt was made on the left side to increase the shunt flow. He became ambulatory with a cane, although the fourth ventricle remained moderately dilated on CT scan. Two months after the additional V - P shunt, he slipped and hit the occiput and immediately became tetraparetic. The pa-tient was treated conservatively under the diagnosis of central spinal cord injury. The MRI taken 2 months af-ter the accident revealed Chiari malformation (type 1), syringomyelia and a dilated fourth ventricle which wascompressing the brainstem. After the fourth ventricu-loperitoneal (FV-P) shunt, the tetraparesis transiently improved but then again worsened. On the CT scan the syrinx did non change in size, while the size of the fourth ventricle became normal. After syringoperitoneal (S - P) shunt the patient showed a moderate improve-ment of tetraparesis. Unfortunately he suffered appen-dicitis complicated with peritonitis and all the shunts were immediately changed to external drainage. However, the patient developed meningitis and became paraplegic. The motor function of the upper extremities slighly improved by aspiration of fluid via the external drainage system from the syrinx. Gardner's Operation was performed to stop the CSF flow from the fourth ventricle. However, the patient died of pneumonia with-out neurological improvement one year later.
We discuss in detail the treatment of DLCFV with syringomyelia and the pathogenesis of the deterioration of syringomyelic symptoms following the FV - P shunt in this case.
Copyright © 1991, Igaku-Shoin Ltd. All rights reserved.

