Japanese
English
- 有料閲覧
- Abstract 文献概要
- 1ページ目 Look Inside
I.はじめに
側頭葉の病変は,身体症状をあらわしにくいが,種々のmental symptomを引き起し得る。これはWilli—ams16,17)が言うように,側頭葉が,あらゆる感覚を統合し,最終的に自己認識を行なう場であるからで,そこには感情とか本能的な感覚や行動,さらには内的外的環境の変化に対する内臓の反応も含まれる。
我々は最近,身体症状が目立たず,mental symptomを前面に呈し,側頭葉に主病変を認めた6症例を経験したので報告する。
Six cases of temporal lobe lesions with prominent mental symptoms and without clear physical signs were reported.
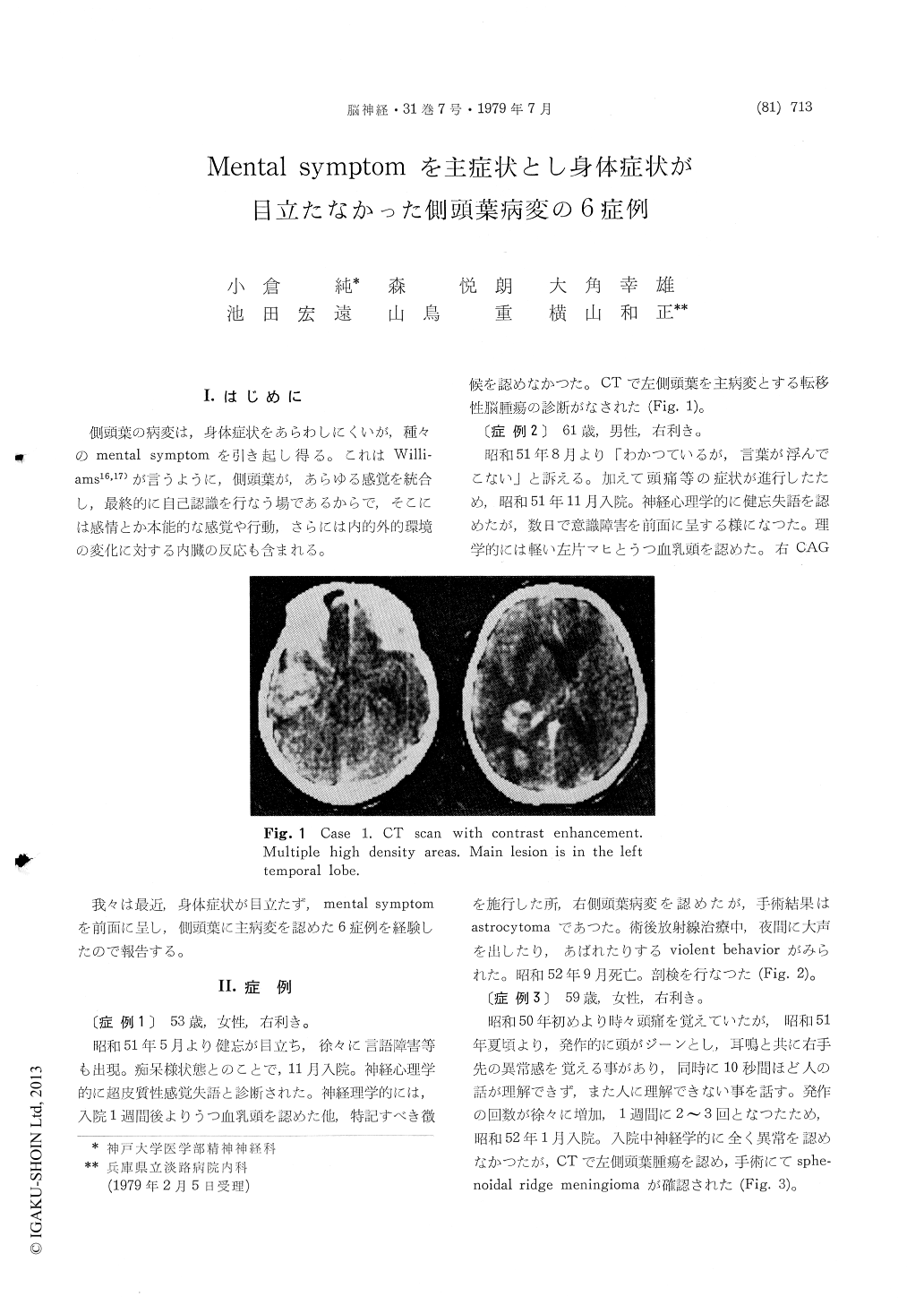
Case one, right handed 53 year-old female, suffered from speech disturbance and impaired mentation. Initial diagnosis had been presenile dementia. But closer examination confirmed the presence of trans-cortical aphasia. With a help of CT scans the final diagnosis of metastatic brain tumor was established with a principal lesion in the left temporal lobe.
Case two, 61 year old right handed male, de-veloped headache, speech disturbance and mild left hemiparesis. Neuropsychological examination re-vealed amnestic aphasia. The patient was operated for astrocytoma which was situated in the right temporal lobe. In subsequent course of radiationtherapy violent behaviors were often observed.
Case three, right handed 59 year-old female, ex-perienced aphasic seizures which were characterized by loss of auditory language comprehension and spontaneous production of incoherent words and would last about 10 seconds. Left sided sphenoidal ridge meningioma was removed by operation.
Case four, right handed 67 year-old female, had a sudden fall followed by nausea, vomiting, headache and confusion. In a hospital she would shriek, got angry and did not cooperate. An autopsy revealed putamenal hemorrhage rupturing into the left temporal lobe.
Case five, right handed 63 year-old man, started to behave abnormally. Agitation and violent behavior were also present. Glioblastoma of the right temporal lobe was found and removed eventually.
Case six, right handed 39 year-old male, had been recovering from the initial infarction of the right temporo-occipital area due to Moyamoyadisease when the second infarction destroyed the left temporooccipital area. Cortical blindness, and oral tendency as well as violent behavior developed.
Thus, aphasia such as transcortical sensory type or amnesic type which was crossed, was major symptoms in the first two cases. These atypical aphasias have to be kept in mind when apparently demented patients were encountered. Aphasic seizure of the case 3 was also unusual but the proper diagnosis pointed to the temporal lobe lesion also. Violent behavior was characteristic in the last three patients. Although responsible structure for violent behavior is still disputed, our present experience suggests importance of temporal lobe lesions.
When patients with prominent mental symptoms but with obscure physical signs are encountered, a possibility of temporal lobe lesion has to be con-sidered.
Copyright © 1979, Igaku-Shoin Ltd. All rights reserved.

