Japanese
English
- 有料閲覧
- Abstract 文献概要
- 1ページ目 Look Inside
I.はじめに
脳硬塞においては髄液が清澄であることが診断基準の1つとされているが,出血性硬塞を随伴する場合には,しばしば血性髄液が採取されることが知られている。しかし,出血性硬塞に関してはその膨大な実験的あるいは病理学的な知見にもかかわらず,いまだ臨床レベルでの把握が充分になされていない。したがって,如何なる脳硬塞症例に血性髄液が認められるかを検討することは,出血性硬塞という病態を臨床的に診断する上にきわめて重要である。
一方,出血性硬塞発症機序に関する実験的報告によれば7,19),閉塞血管の再開通が大いに関与していることが示唆されている。それにもかかわらず脳血管写で再開通を確認した脳硬塞臨床例についての髄液色調を観察した報告も少なく,出血性硬塞あるいは血性髄液の発現に関してはこのような再開通例での検討もまた必要となつてくる。
Even, in the patients with ischemic cerebro-vascular diseases the cerebrospinal fluid (CSF) be-comes sanguinous when the patients developedhemorrhagic infarction. However, despite a largenumber of reports on the hemorrhagic infarctionthrough animal experiments or pathological studies,the clinical comprehension of hemorrhagic infarc-tion has not been established. Thus to obtain moreaccurate diagnosis of stroke patients it is most im-portant to know what kinds of infarcted patientsdevelope sanguinous fluid. The present study wasdesigned to inspect the occurrence of sanguinousor xanthochromic CSF in the patients who werediagnosed as cerebral infarction following bothphysical and angiographical findings within 24 hoursafter the beginning of the symptomes. And thestudy was also performed with special reference tothe occurrence of recanalization of the occludedartery, which has been experimentally suggestedas being correlated to the developement of hem-orrhagic infarction.
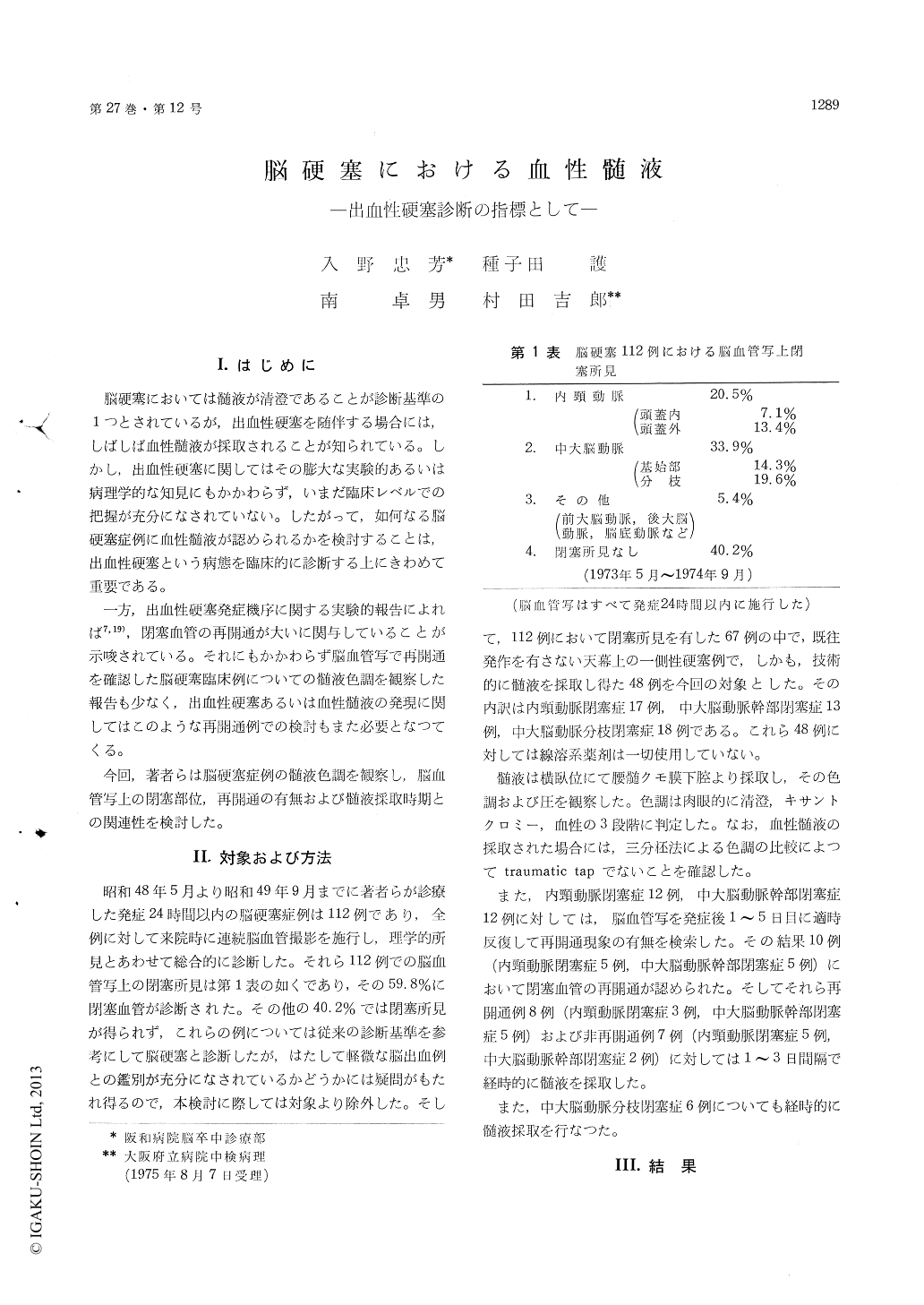
Among 112 infarcted patients 49 demonstratedarterial occlusion on the angiograms obtained within24 hours after the onset were selected for thepresent study. These 49 patients comprised 13with the internal carotid artery occlusion, 18 withthe middle cerebral arterial axis occlusion and 18with the occlusion of the smaller branch of middlecerebral artery. Fibrinolytic agents were not usedfor the treatment of them. The colour of the fluidobtained by lumbar puncture was estimated as clear,xanthochromic and sanguinous. In 8 of internalcarotid artery occlusion, 7 middle cerebral arterialaxis occlusion and 5 middle cerebral arterial branchocclusion the CSF was obtained consecutively atone- to three- day intervals in the first week. And7 and 8 cases with the internal or the middlecerebral arterial axis occlusion were performedfollow-up angiographies between one- to five- dayintervals to check the recanalization. All of theresults of CSF and angiographical findings werecompared each other.
The fluid was clear in all of 49 infarcted patientswithin 24 hours after the onset except for 2 caseswith the middle cerebral arterial branch occlusion.Consecutive lumbar puncture displayed the de-velopement of sanguinous or xanthochromic CSFin 7 of 15 with internal carotid of middle cerebralarterial axis occlusion after 2 or 3 days after theonset, while none of 5 with middle cerebral arterialbranch occlusion developed abnoramal appearancein their course within a first week. The sanguinousfluid was apt to appear more frequently in therecanalized cases, i. e. 6 among 8 recanalized and 1among 7 non-recanalized. Five fatal cases withrecanalization were autopsied and certificated asdisplaying hemorrhagic infarction.
From the above data it is apparent that hem-orrhagic infarction frequently developes after majorcerebral arterial occlusion, especially in those show-ing angiographical recanalization. It is essestialfor the clinicians to perform consecutive lumbarpunctures to diagnose hemorrhagic infarction. Itmight be true that spontaneous recanalization wouldprovide poorer prognosis for the infarcted patientsby enhancing the developement of hemorrhagic in-farction like the animal experiments which sug-gested that the recanalization of the occluded arterycorrelated to the developement of hemorrhagic in-farction.
Copyright © 1975, Igaku-Shoin Ltd. All rights reserved.

