Japanese
English
- 有料閲覧
- Abstract 文献概要
- 1ページ目 Look Inside
はじめに
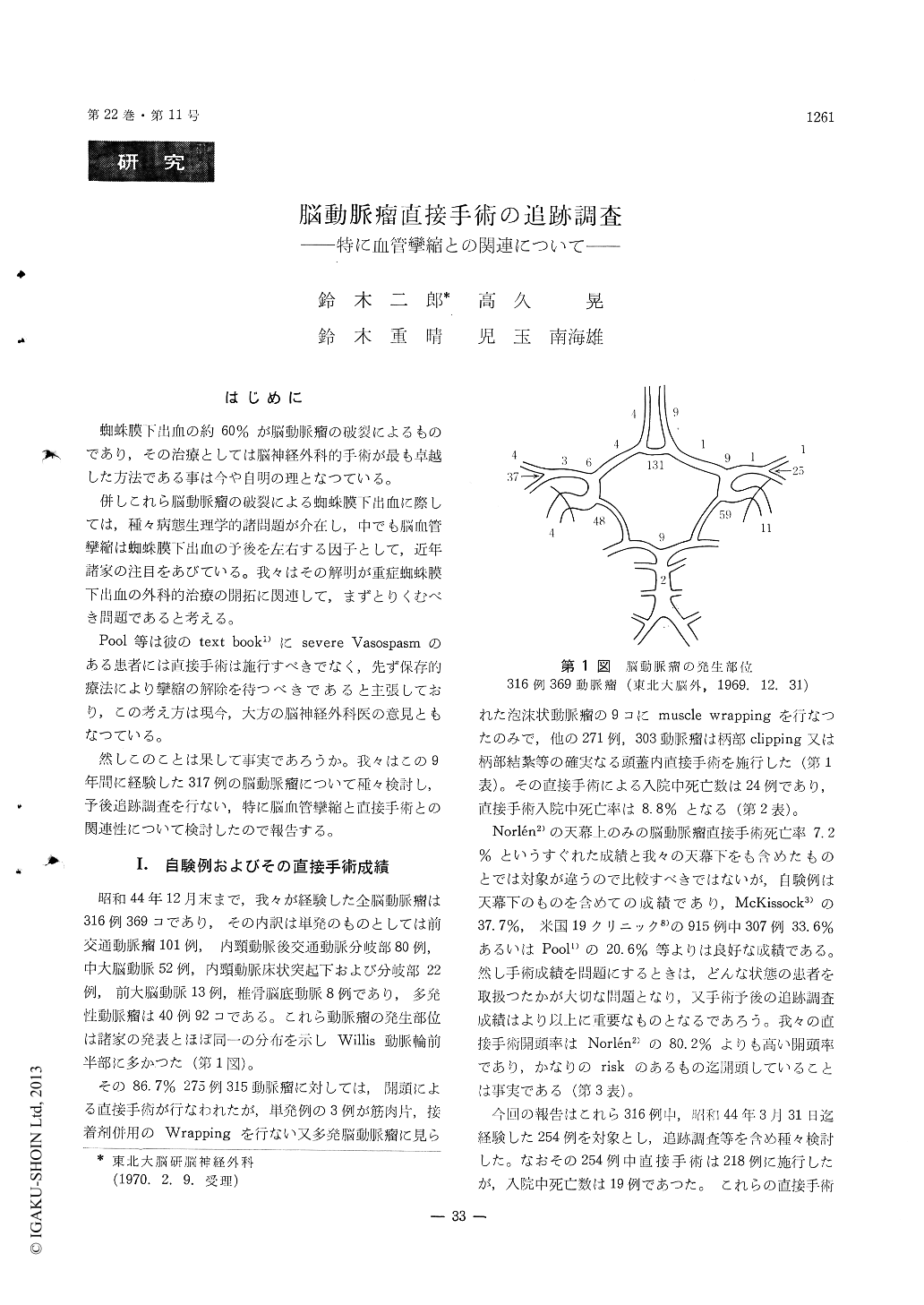
蜘蛛膜下出血の約60%が脳動脈瘤の破裂によるものであり,その治療としては脳神経外科的手術が最も卓越した方法である事は今や自明の理となっている。
併しこれら脳動脈瘤の破裂による蜘蛛膜下出血に際しては,種々病態生理学的諸問題が介在し,中でも脳血管攣縮は蜘蛛膜下出血の予後を左右する因子として,近年諸家の注目をあびている。我々はその解明が重症蜘蛛膜下出血の外科的治療の開拓に関連して,まずとりくむべき問題であると考える。
1) Direct operation were performed in 218 cases out of 254 cases of intracranial aneurysm we have experienced until the end of March, 1969. The follow up study which is made during hospitaliza-tion after operation, 3 cases in which patients died within 6 months after operation (one case died of severe hepatitis, and one case gastric cancer), 3 cases in which patients died in more than 6 month and 192 cases in which patients are surviving for 6 months after operation the survival rate for 6 months accounts for 90. 6%.
2) There were 61 vasospasm cases, in 44 cases of which vasospasm was found before the operation including that of non-operative cases, and in 17 cases of them vasospasm was found only after the opera-tion. The occurrence rate of vasospasm was 17. 3%.
3) As for vasospasm cases, there was no case in which operated patient died within 6 months after operation, while there were only two cases out of 37 cases in which patients died during hospitaliza-tion, the mortality rate being 5. 4%. We could find two cases in which patients had had major deficit since before the operation and still had though progressing favourably. While in non-vasospasm cases the mortality rate within 6 month after opera-tion was 10. 2%. There is little difference between the result of vasospasm cases and that of non-vasospasm cases.
4) The above mentioned follow up study brought us to reconsider to some extent the view that in severe vasospasm cases direct operation should not be performed. In vasospasm cases in which, unless the patients are in coma or are taking a down hill course, direct operation should be performed with tender care without giving damage to brain, especi-ally when the level of consciousness is not variable or is rising in a steady curve.
5) We are of the opinion that after treating the dangerous aneurysm we should use vasodilator, thus making cerebral blood flow better and should carry rehabilitation into effect at an earlier stage.
Copyright © 1970, Igaku-Shoin Ltd. All rights reserved.

