Japanese
English
- 有料閲覧
- Abstract 文献概要
- 1ページ目 Look Inside
I.はじめに
内頸動脈海綿静脈洞瘻は比較的稀な疾患であり,Sed—zimirら22)は頭蓋内動脈瘤669例中に1例,cranio-facial injury 1100例中に3例の本症を認めたと報告している。成因について,PoolおよびPotts19)によれば,その70%が外傷性内頸動脈壁損傷であり,その他は先天性または動脈硬化性の海綿静脈洞部内頸動脈瘤の破裂したものであると言われている。
症状は動脈血が直接海綿静脈洞内に流入するための搏動性眼球突出,頭蓋内雑音,眼筋麻痺,視力障害などにより特徴づけられるが,中には非定型的な症状を示す例も報告されており,診断には頸動脈写像に動静脈瘻を確認する必要がある。
Three casee of carotid-cavernous fistula of trau-matic origin are reported and etiology of postopera-tive visual disturbance and its prevention are discussed in the present report.
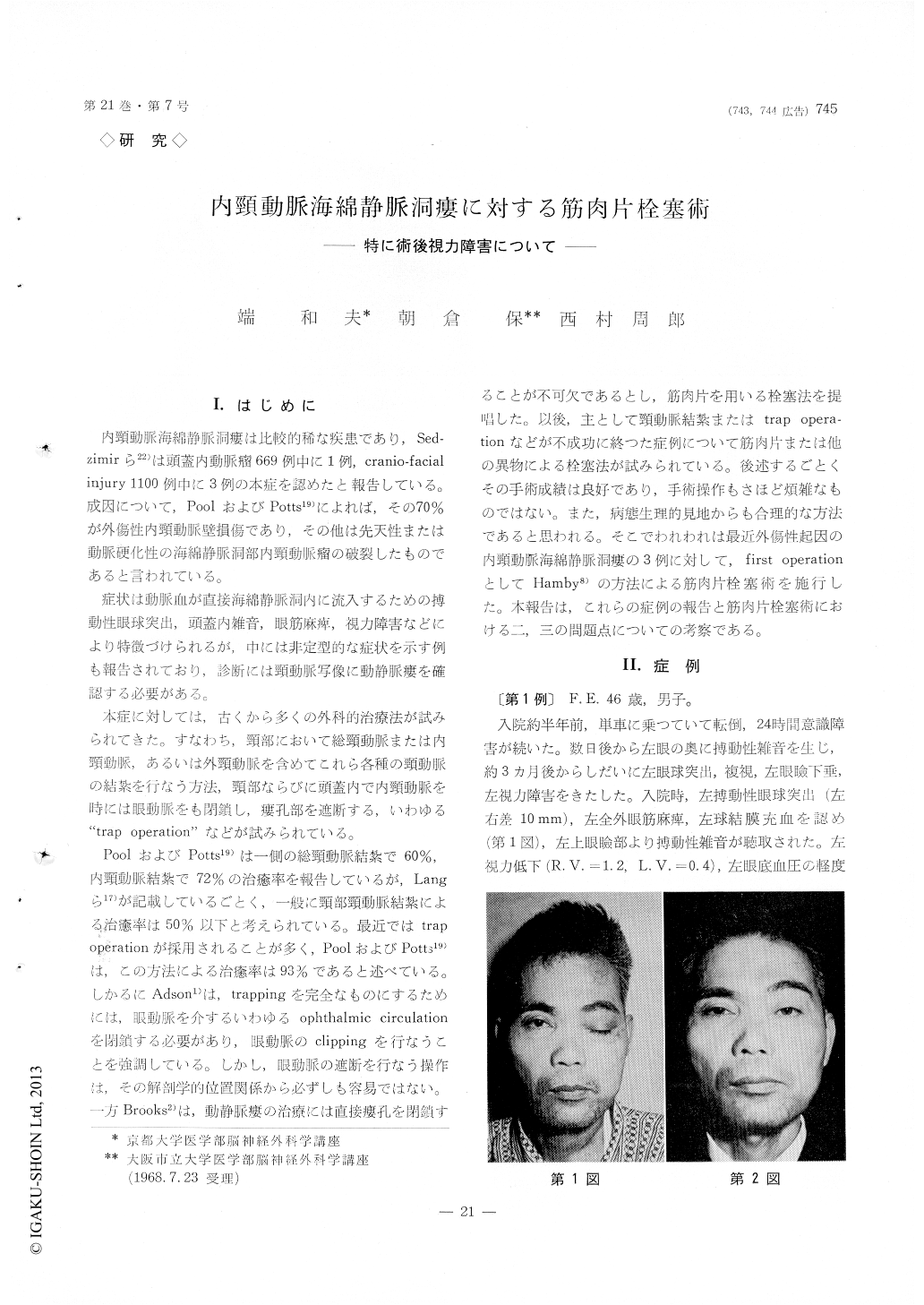
In the first case, 46-year-old male, bruit was noted behind the left eye several days after the trauma. Exophthalmos, diplopia, ptosis of the upper eyelid and visual disturbance developed three months after the injury. In the second case, 26-year-old female, bruit in the frontal region and swelling of the eyelid on the right side were noted several hours after the traffic accident. Six months later, when she was on the first delivery, exophthalmos and diplopia appeared. In the third case, 9-year-old boy, exoph-thalmos on his right eye appeared ten days after the head injury.
In all cases muscle embolization with trapping of fistulous lesion was performed. First of all, intracra-nial clipping was made on the chiasmatic portion of the internal carotid artery. Then the external, internal and common carotid arteries were exposed in the neck. Muscle sticks, measuring 0.3×0.3×2 cm, were introduced into the internal carotid artery through a small incision on the external carotid artery, and were propelled by the blood stream of the internal carotid artery to the fistulous lesion. The external and internal carotid artery were then ligated.
After the operation, exophthalmos, diplopia and swelling and chemosis of the eyelids have disap-peared completely in all cases. In the first and second case, however, visual disturbance was noted postoperatively.
Muscle embolization with trapping of the fistulous portion is the best procedure for the treatment of this kind of lesion. Neither cervical carotid ligation nor intracranial trapping procedure alone can make good result in almost all cases having carotid-cavernous fistula. The reason is as follows : 1) Liga-tion of the common or internal carotid artery in the neck in dangerous, because it not only deprives the blood supply to the brain of the ligated side but also steals blood from the opposite carotid clown into the fistulous opening, followed by ischemia of the brain. 2) Carotid trapping even including liga-tion of the ophthalmic artery can not always make satisfactory result, because there are many arterial branches around the cavernous portion of the in-ternal carotid artery and flow through these branches will leave the fistula persistent.
Therefore, muscle embolization technique with trapping procedure should be performed as the primary definitive surgery.
In the first case, after the surgery, bruit on the left eyelid disappeared objectively, though the fistula was still demonstrated by right carotid angiography. Therefore, disappearance of bruit can not be a good index of complete obliteration of the fistula. Internal carotid angiography should be performed during surgery in order to a certain occlusion of the fistula.
In two out of three cases, severe visual disturbance developed postoperatively. In these cases ophthal-modyinamometry showed a significant postoperative decrease of the blood pressure of the optic artery. It can be assumed that the circulatory failure of the ophthalmic artery may be responsible for visual disturbance. It is reasonable to assume that incom-plete obliteration of the fistulous opening may result in a reversal of flow in the ophthalmic artery, and hence the blood supply to the retinal arteries, being end arteries, may be decreased. In order to prevent the visual disturbance after surgery, complete oblite-ration of the fistula will be required. Furthermore, at surgery, it is worth trying to preserve flow of the external carotid artery, for keeping retrograde blood supply to the ophthalmic artery through the external carotid system.
Copyright © 1969, Igaku-Shoin Ltd. All rights reserved.

