Japanese
English
- 有料閲覧
- Abstract 文献概要
- 1ページ目 Look Inside
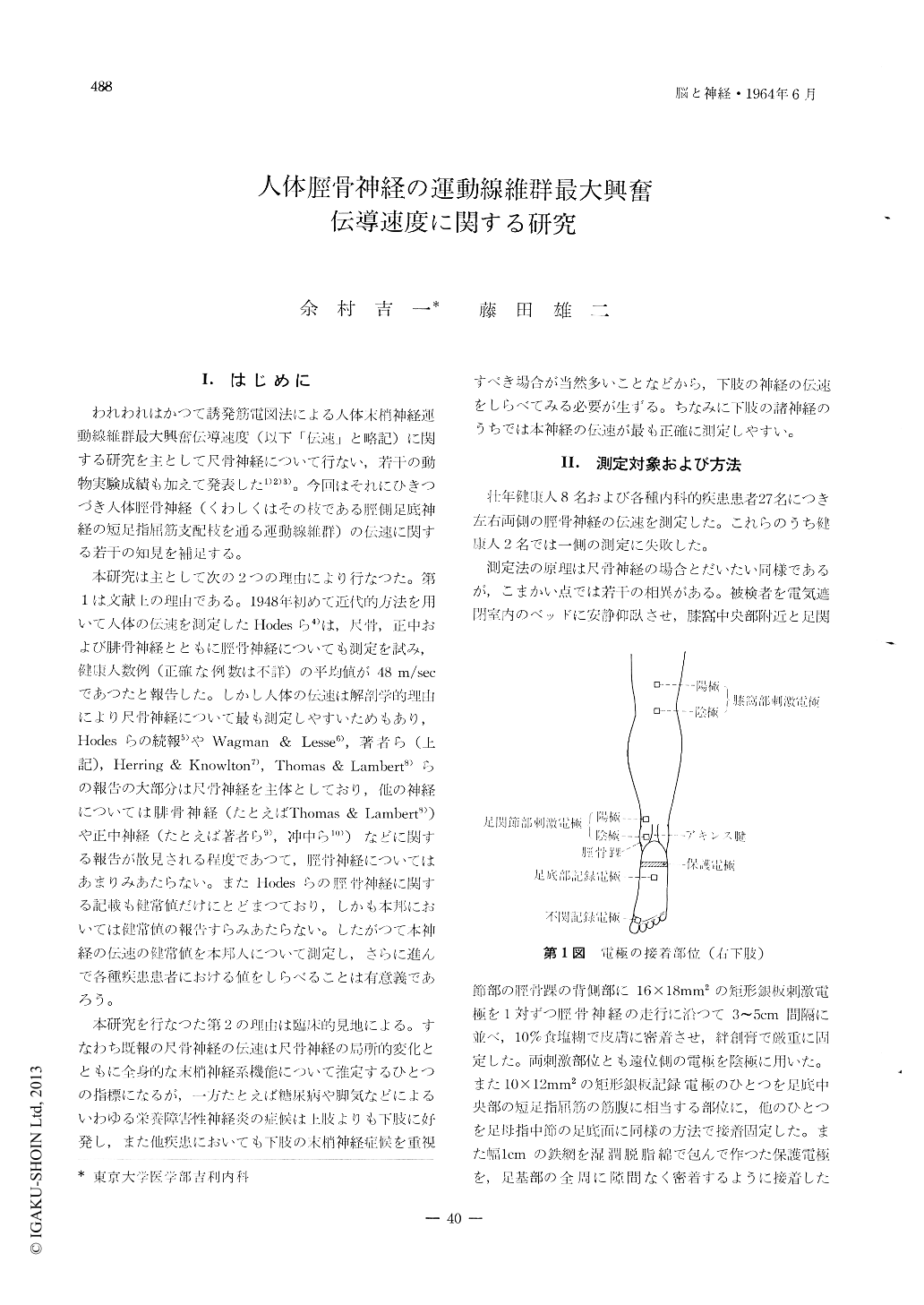
1)誘発筋電図法により人体脛骨神経(くわしくはその枝である脛側足底神経の短足指屈筋支配枝)の運動線維群の最大興蕾伝導速度(伝速)を測定した。
2)経皮的刺激閾値は尺骨神経の伝速測定時よりも一般に高く,若干の測定失敗例もあつたが,成功例の大多数では測定の指標となるM波の波形は2相性であり,F波は痕跡的にみられ,H波は全然みられなかつた。足底部の記録電極の接着部位を移動すると,M波の性状が著明に変化した。
3)壮年健康人における測定値は47.8±4.3m/sec(N=14)であり,危険率1%で左右差なく,既報の尺骨神経伝速の健常値63.6±6.0m/sec (N=54)にくらべ明かに低値であつた。分布範囲は40.9〜57.4m/secであつた。
4)末梢性単麻痺,急性灰白髄炎後遺症,筋萎縮性側索硬化症,脊髄空洞症,Jacksonてんかん,片麻痺,進行性筋ジストロフィー,糖尿病,慢性腎炎,甲状腺機能兀進症,慢性腸炎,胃癌,再生不良性貧血,肥腔症,肝硬変などの各種内科的疾患患者27例の左右の脛骨神経伝速を測定したが,個々の測定値で健常値分布範囲を著明に逸脱したものはなかつた。
5)統計的には糖尿病(危険率1%)と慢性腎炎(同5%)で健康人にくらべて脛骨神経伝達の有意低下がみられ,筋萎縮性側索硬化症,片麻痺,甲状腺機能亢進症慢性腸炎などではそれがみられなかつた。
Measurement was made of the maximum impulse conduction velocity in motor fibers of the human tibial nerve (more precisely to say, the motor fibers which innervate the flexor digitorum brevis muscle through the medial plantar nerve) by giving electrical shocks to the nerve percutaneously at the popliteal and ankle joint regions and by deriving evoked potentials from the central region of the sole. The threshold against stimulation was considerably higher than in the case of stimulating the ulnar nerve. The M wave was biphasic and the F wave was very small in most cases. The H wave was never observed.
The condcction velocity in 14 tibial nerves in 8 normal subjects distributed from 40.9 to 57.4 m/sec with a mean of 47.8 and a standard deviation of ±4.3 There was no significant difference between conduction velocities on the both sides, and the mean was considerably smaller than that of the conduction velocities in normal ulnar nerves on which we reported previously. No extreme abnormality was encountered in any individual value of the con-duction velocities in bilateral tibial nerves in 27 patients with peripheral monoplegia, sequelae of acute anterior poliomyelitis, amyotrophic lateral sclerosis, syringomyelia, Jacksonian epilepsy, hemiplegia, pro-gressive muscular dystrophy, diabetes mellitus, chronic nephritis, hyperthyroidism, chronic entero-colitis, gastric cancer, hypoplastic anemia, obesity, liver cirrhosis etc. On statistical calculation, the conduction velocity was significantly slower than normal in diabetes mellitus and chronic nephritis, but it was normal in amyotrophic lateral sclerosis, hemiplegia, hyperthyroldism and chronic enterocolitis.
Copyright © 1964, Igaku-Shoin Ltd. All rights reserved.

