Japanese
English
- 有料閲覧
- Abstract 文献概要
- 1ページ目 Look Inside
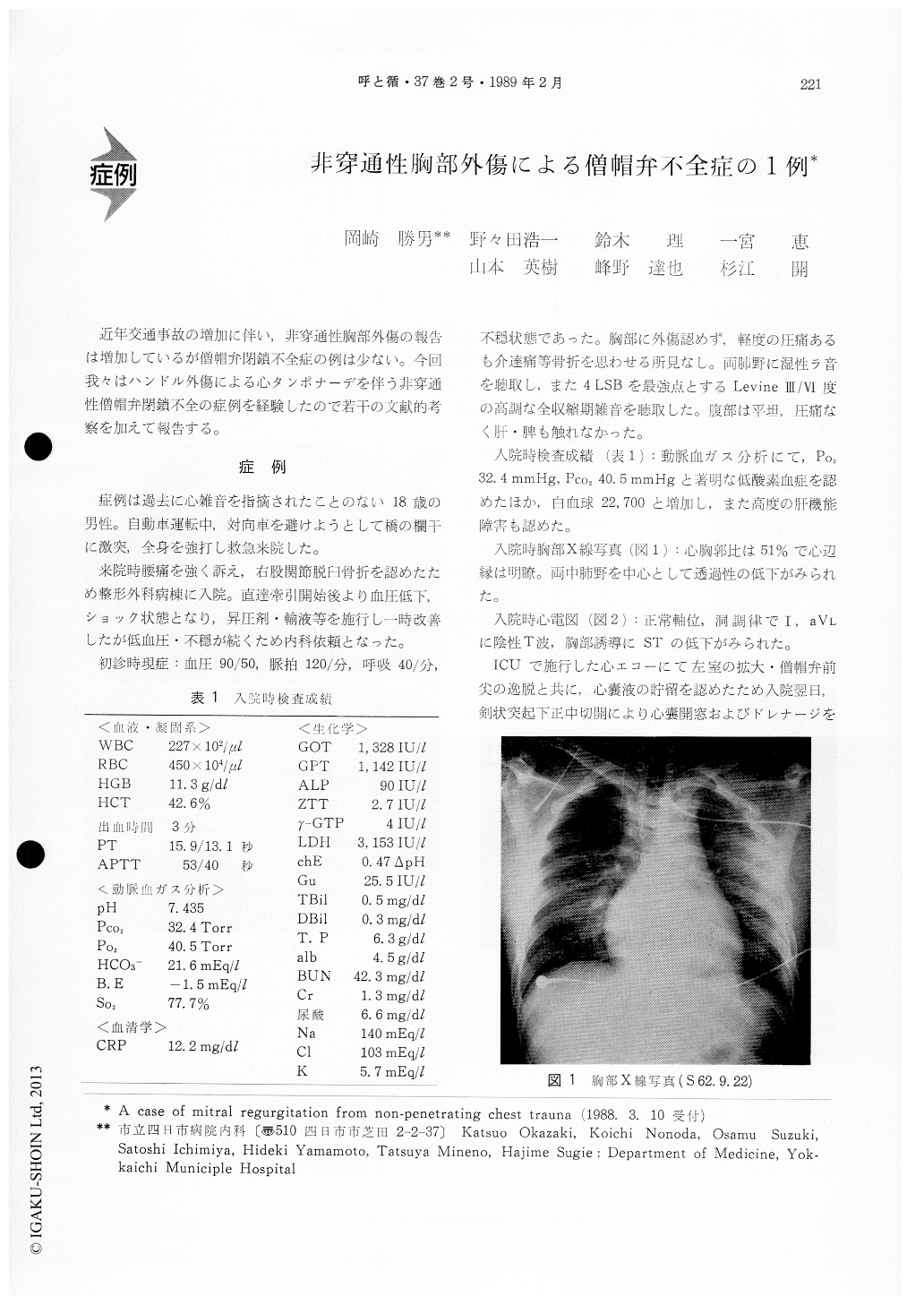
近年交通事故の増加に伴い,非穿通性胸部外傷の報告は増加しているが僧帽弁閉鎖不全症の例は少ない。今回我々はハンドル外傷による心タンポナーデを伴う非穿通性僧帽弁閉鎖不全の症例を経験したので若干の文献的考察を加えて報告する。
A 18-year-old boy, with no evidence of cardiac murmurs in the past, was admitted to our hospital after steering wheel injury on Nov 22, 1987. He im-mediately became in shock state.
Physical examination revealed a grade 3/6 apical holosystelic murmur and moist rales in lungs. Two-dimensional echocardiography showed a prolapsed anterior leaflet and a lot of pericardial effusion. Herecovered soon after subxiphoid pericardiotomy, then we obtained bloody fluid of 200 m/.
In cardiac catheterization study, the pulmonary artery wedge pressure was elevated with a V-wave of 31 mmHg.
Coronary angiogram, right ventriogram, and aort-ogram were normal, but left ventriography revealed grade 4 (Seller's) mitral regurgitation.
Mitral valve replacement was performed with a Bjork-Shiley prosthesis on Feb 8, 1988. Anterior papillary muscle was in a white necrosis, but not raptured. Mitral valve leaflets and chordae tendanace were intact.
12 cases of mitral regurgitation from non-penetra-ting blunt chest trauma were reported in Japan, but we first report a case of mitral regurgitation due to non-ruptured papillary muscle dysfunction.
Copyright © 1989, Igaku-Shoin Ltd. All rights reserved.

