Japanese
English
- 有料閲覧
- Abstract 文献概要
- 1ページ目 Look Inside
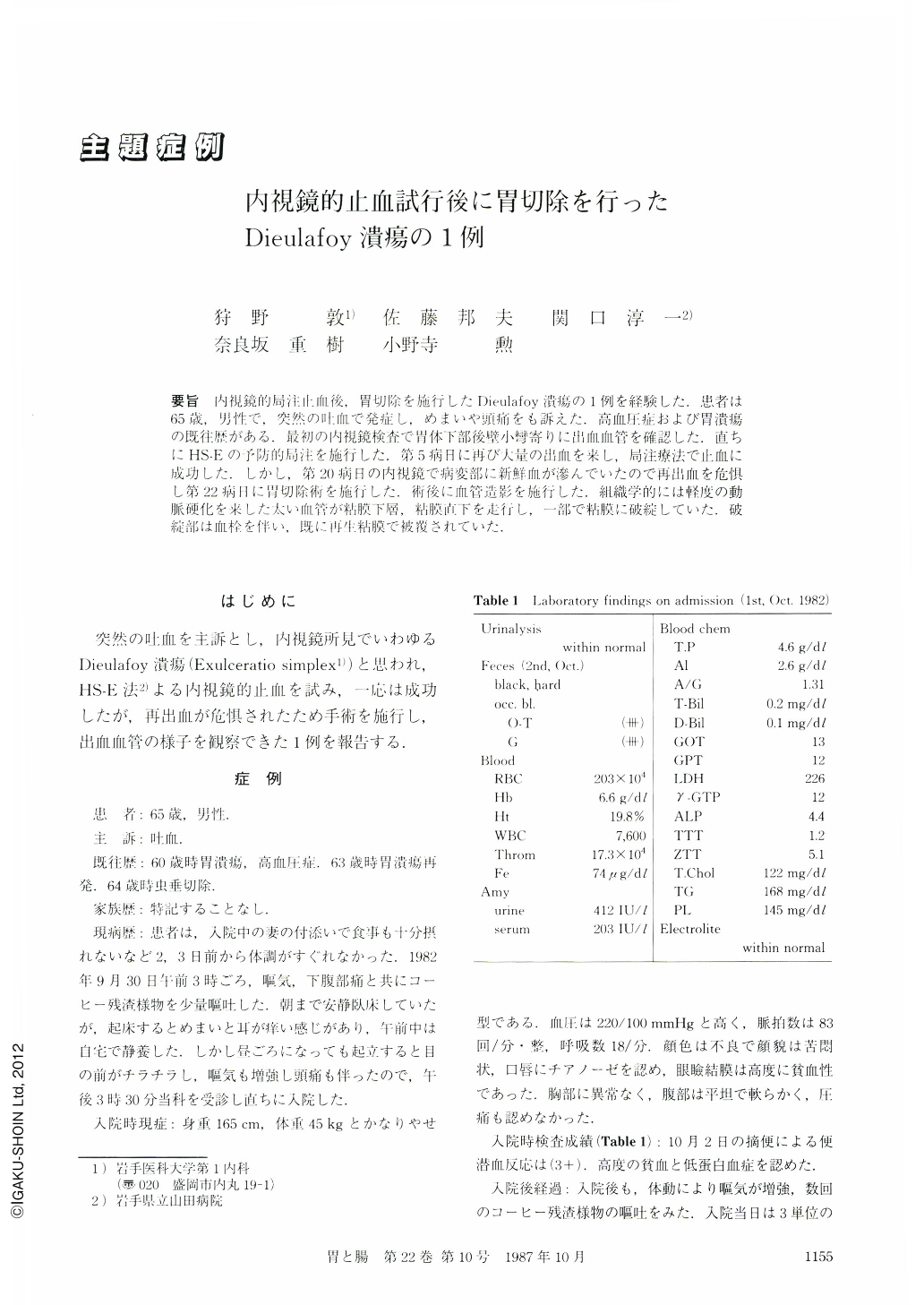
要旨 内視鏡的局注止血後,胃切除を施行したDieulafoy潰瘍の1例を経験した.患者は65歳,男性で,突然の吐血で発症し,めまいや頭痛をも訴えた.高血圧症および胃潰瘍の既往歴がある.最初の内視鏡検査で胃体下部後壁小彎寄りに出血血管を確認した.直ちにHS-Eの予防的局注を施行した.第5病日に再び大量の出血を来し,局注療法で止血に成功した.しかし,第20病日の内視鏡で病変部に新鮮血が滲んでいたので再出血を危惧し第22病日に胃切除術を施行した.術後に血管造影を施行した.組織学的には軽度の動脈硬化を来した太い血管が粘膜下層,粘膜直下を走行し,一部で粘膜に破綻していた.破綻部は血栓を伴い,既に再生粘膜で被覆されていた.
We experienced a case of Dieulafoy's urcer in which endoscopic hemostasis was performed before gastrectomy. A 65-year-old male with a past history of hypertension and gastric ulcer suffered from a sudden onset of hematemesis. He complained of vertigo and headache on admission. In the first endoscopic examination (Fig. 1), a small blood clot was observed on the posterior wall of the lower gastric body. Endoscopic hemostasis was immediately conducted for the prophylactic purpose using HS-E method. However, massive rebleeding occurred on the 5th hospital day (Fig. 3). Endoscopic hemostasis was successfully done again. Oozing of fresh blood from the lesion was again recognized endoscopically on the 20th hospital day (Fig. 6) and gastrectomy was performed prophylactically on the 22nd hospital day. Angiography was conducted postoperatively.
Histological examination revealed a large artery running in the submucosa just under the mucosa (Fig. 9a). A ruptured part of the vessel filled with thrombus was covered with fibrosis and regenerative mucosa (Fig. 9b).
Copyright © 1987, Igaku-Shoin Ltd. All rights reserved.

