Japanese
English
- 有料閲覧
- Abstract 文献概要
- 1ページ目 Look Inside
本邦における大腸憩室病は,現在,欧米並みの頻度で報告されている.欧米とは異なり,右側大腸に多いこと,および欧米の成書,報告(文献)にみるような重篤な合併症が少ないことが周知になっている.
We had 244 cases of diverticular disease. All of them were studied radiologically. Six cases were operated and 10 cases were studied in autpsy. In addition, we studied about 73 cases which were reported as diverticulitis in the literatures. The results were as following;
1. Pathological findings: The 10 cases which were studied in autopsy had 66 diverticula. Moderate inflammatory changes were recognized in 9.1% (6 out of 66 diverticula). But, the patients of these cases had no abdominal symptoms. The circulars muscle was 2.2~2.5 mm in sigmoid diverticular disease, and 0.9~1.0 mm in coecum and ascending colon diverticular disease.
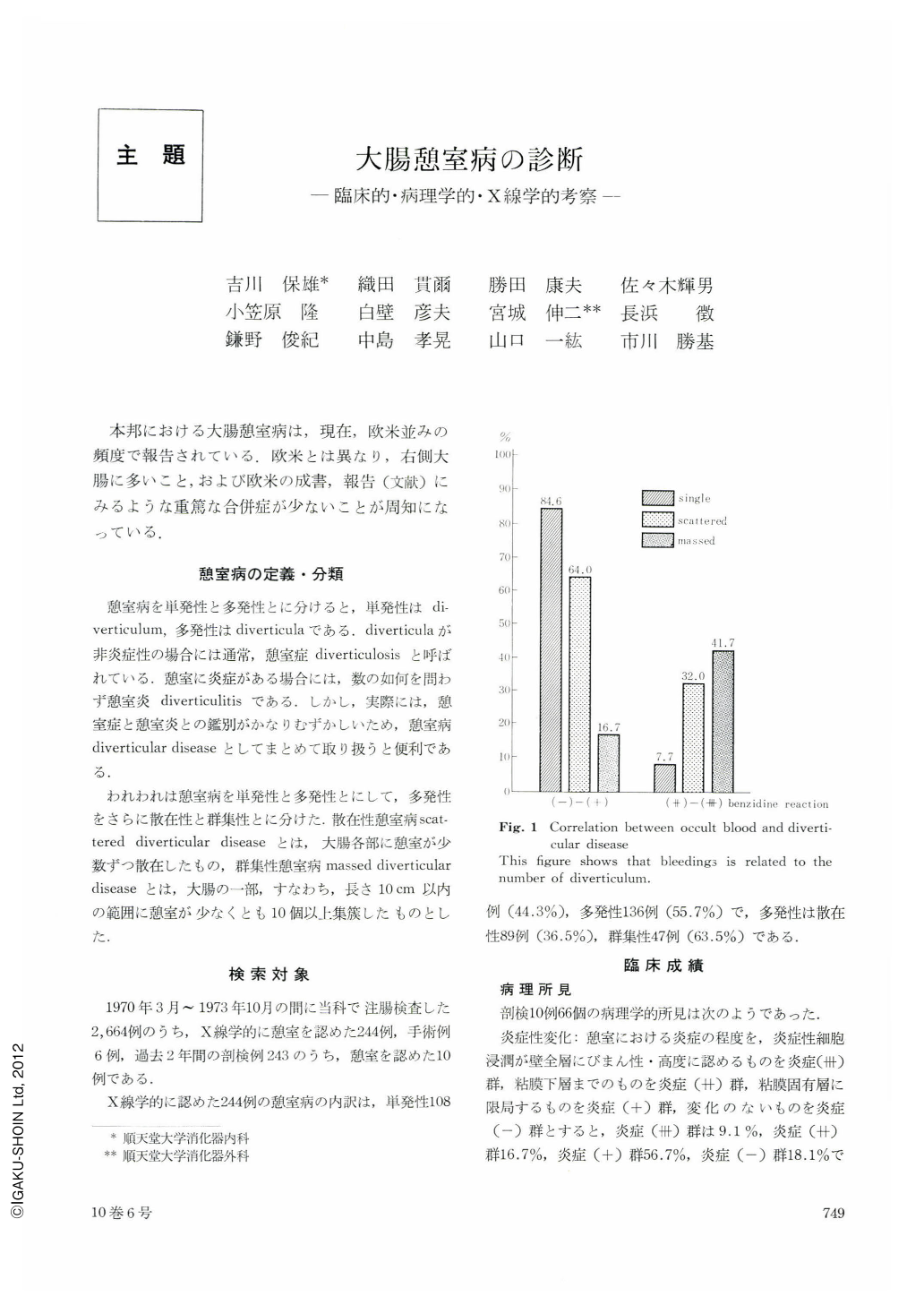
2. Clinical findings: Leucocytosis was recognized in 2.6% of single, 3.4% of scattered and 0% of massed diverticular disease. But no relation with diverticulitis was found. Bloody stool was observed in 0% of single, 5.2% of scattered and 17.2% of massed diverticular disease. Occult blood was recognized in 84.6% of single, 64.0% of scattered and 16.7% of massed diverticular disease in the group of benzidine reaction (-)~(+). But, in the group of benzidine reaction(++)~(+++), occult blood was recognized in 7.7% of single, 32.0% of scattered and 41.7% of massed diverticular disease. In other words, bloody stool and occult bleeding were related to the number of diverticulum. Tumor-like resistence was noted in 1.3% of single, 3.4% of scattered and 24.1% of massed diverticular disease. That is, this had close relation with massed diverticular disease. Tenderness was noted in 1.3% of single, 17.2% of scattered and 27.6% of massed diverticular disease. Localized tenderness was related to the number of diverticulum, Diarrhoea and/or constipation had no relation with the number or inflammatory change of diverticulum.
3. X-ray findings: Massed diverticular disease showed haustral irregularity in 84.1%, limited distensibility in 70.5%, asymmetrical or crowded folds in 59.1% and marginal irregularity in 50.5%. On the other hand, scattered diverticular disease showed haustral irregularity in 41.4%, limited distensibility in 18.6%, asymmetrical or crowded folds in 11.4% and marginal irregularity in 4.3%. Single diverticulum showed almost no change.
We compared the differences between the right-sided and the left-sided massed diverticular disease. The following data are shown about (a) the right-sided colon and (b) the left-sided colon. Marginal irregularity: (a) 36.7%, 78.6%, haustral irregularity: (a) 43.3%, (b) 85.7%, limited distensibility: (a) 56.7%, (b) 78.6%, crowded folds: (a) 43.3%, (b) 85.7%, and asymmetrical folds: (a) 6.7%, (b) 57.1%. The differences of x-ray findings between right-sided and left-sided massd diverticular disease could be caused by the difference of muscular thickening.
In addition, we studied about 73 cases of diverticulitis reported in the literature (12 cases in the right-sided and 61 cases in the left-sided colon), and compared the differences of x-ray finding between the right-sided (a) and the left-sided (b) diverticulitis. Marginal irregularity: (a) 58.3%, (b) 65.6%, deformity: (a) 33.3%, (b) 85.2%, limited distensibility: (a) 66.7%, (b) 82.0%, crowded folds: (a) 8.3%, (b) 29.5%, irregular folds: (a) 41.7%, (b) 54.0%, cushion-like defect: (a) 58.3%, (b) 52.5%, fistula: (a) 0%, (b) 57.4%, abscess-cabity: (a) 0%, (b) 39.3%, and barium fleck: (a) 8.3%, (b) 19.7%. It is the prominent features that barium leakage like fistula and abscess-cabity is not noticed in the right-sided colon.
In the literature, it is mentioned that more than half of diverticulitis had only one attack. We think that diverticulitis should still be regarded as a medical diseases until complication make surgical treatment necessary.
Copyright © 1975, Igaku-Shoin Ltd. All rights reserved.

