Japanese
English
- 有料閲覧
- Abstract 文献概要
- 1ページ目 Look Inside
- サイト内被引用 Cited by
胃には噴門と幽門という2つの門がある.幽門はピロルス(門番)であるが,「幽」の字は火の消えるさまをあらわす「ほのぐらい」とか「かすかな」という意味があり,細くせまくなってゆくということをあらわす言葉である.必要に応じて門の開閉を行う門番(ピロルス)という言葉もなかなかうがった表現ではある.
噴門はカルディアともいわれているが,噴門のほうがはるかにいい言葉である.噴門はもともと「ホン」(息を急にふき出す音)からきたもので噴出する門ということになる.「Cardi」は「心(しん)」の意味で「胃の心(しん)に接する部分」ということから噴門とcardiaが同じ場所に用いられるようになったのであろう.
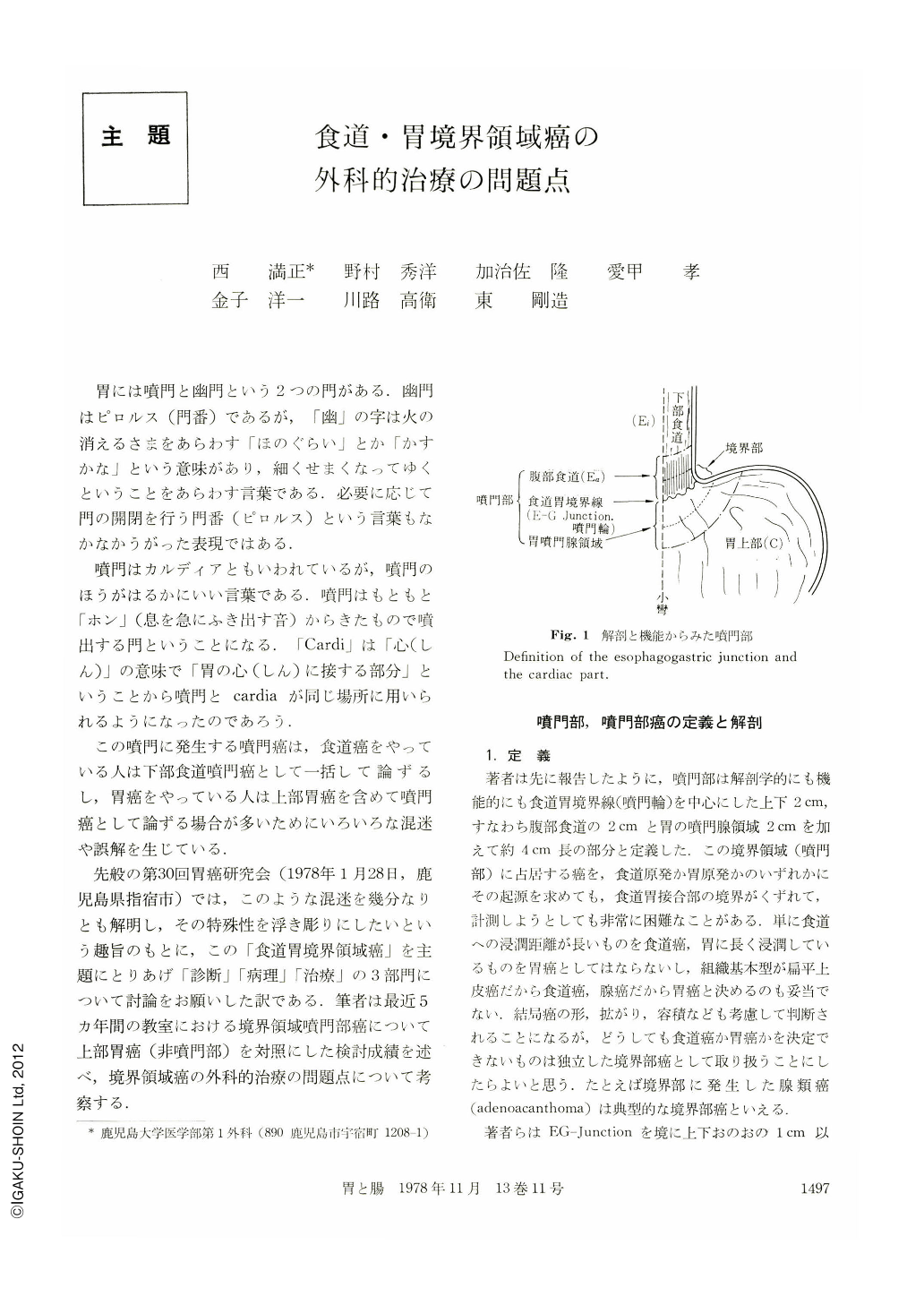
Carcinoma in the esophago-gastric junction (EG junction) and in the cardia are defined as a carcinoma located within 1 cm and 2 cm respectively from EG junction.
Clinical specific feature, problem of preoperative diagnosis, operation method and prognosis have been compared between carcinoma in EG junction and in cardia. Specific features of carcinoma in EG junction are as follows: histologically 15% of cases being squamous cell carcinoma and remaining most of cases showing well differentiated adenocarcinoma; most of early cancer detected preoperatively being protruded type; most of advanced cancer being confined type and frequently seen in aged male. Carcinoma located in the cardia has following features: frequently arising in young female; infiltrative type; histologically undifferentiated type and histology demonstrating invasion to esophagus being more extensive than macroscopic finding.
If preoperative diagnosis indicating esophageal invasion in those carcinomas is more than 2 cm, open chest surgery is required for curative resection, complete lymph node dissection and anastomosis. Line of esophageal transection should be 2 cm oral from tumor in confined type and 4 cm in infiltrative type in order to prevent recurrence. In our department reconstruction of the GI tract has been performed according to double tract N anastomosis. Prognosis after the operation is better in cardiac carcinoma than in carcinoma in the upper portion of the stomach.
Copyright © 1978, Igaku-Shoin Ltd. All rights reserved.

