Japanese
English
- 有料閲覧
- Abstract 文献概要
- 1ページ目 Look Inside
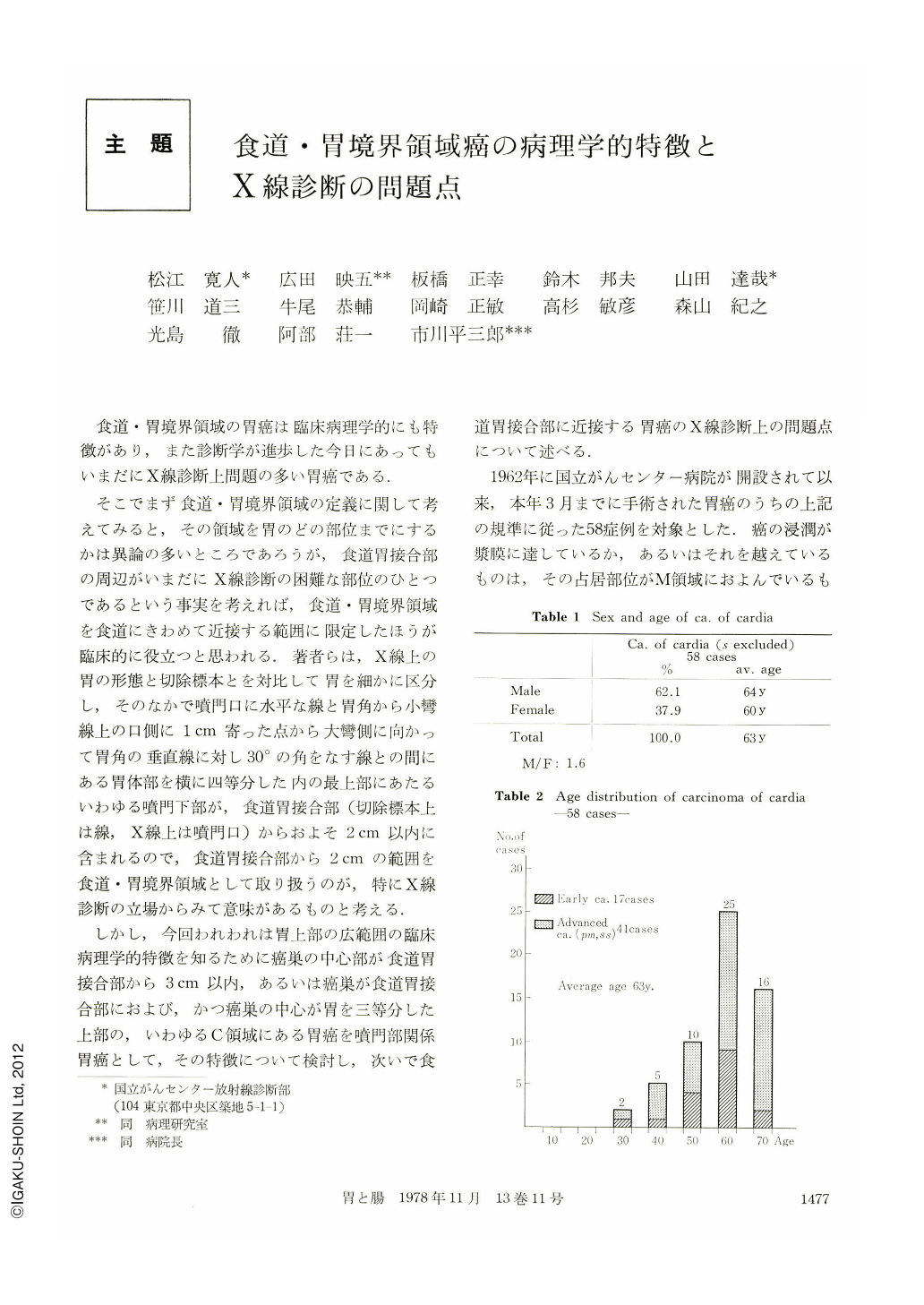
食道・胃境界領域の胃癌は臨床病理学的にも特徴があり,また診断学が進歩した今日にあってもいまだにX線診断上問題の多い胃癌である.
そこでまず食道・胃境界領域の定義に関して考えてみると,その領域を胃のどの部位までにするかは異論の多いところであろうが,食道胃接合部の周辺がいまだにX線診断の困難な部位のひとつであるという事実を考えれば,食道・胃境界領域を食道にきわめて近接する範囲に限定したほうが臨床的に役立つと思われる.著者らは,X線上の胃の形態と切除標本とを対比して胃を細かに区分し,そのなかで噴門口に水平な線と胃角から小彎線上の口側に1cm寄った点から大彎側に向かって胃角の垂直線に対し30°の角をなす線との間にある胃体部を横に四等分した内の最上部にあたるいわゆる噴門下部が,食道胃接合部(切除標本上は線,X線上は噴門口)からおよそ2cm以内に含まれるので,食道胃接合部から2cmの範囲を食道・胃境界領域として取り扱うのが,特にX線診断の立場からみて意味があるものと考える.
Age of gastric cancer cases of esophago-cardiac region is statistically higher than all of gastric cancer cases. They show mostly macroscopical forms of localized and elevated type of lesions, that are Borr. 2 type in advanced gastric cancer or Ⅰ, Ⅱa type in early gastric cancer. Histologically most of them appear well differentiated adenocarcinoma. Concerning to the form of depth infiltration, we have classified them into expansive type, scattered infiltrative type and diffuse infiltrative type. Over 80% of gastric cancer of the esophago-cardiac region were classified as expansive type. Therefore X-ray diagnosis of cancer of the esophago-cardiac region is not so difficult, because they show localized tumors distinguished clearly from surrounding normal tissue with good extension by double contrast method.
However, the cases of operated early gastric cancer of the esophago-cardiac region is fairly few compared with advanced gastric cancer in the same region.
The radiological techniques and diagnosis of the esophagocardiac region have already progressed, but they have not been used so effectively in the cases of the esophago-cardiac region that some cases of early gastric cancer may be missed even with double contrast method. So, some kinds of radiological technique of esophago-cardiac region should be seriously taken in routine X-ray examination.
Copyright © 1978, Igaku-Shoin Ltd. All rights reserved.

