Japanese
English
- 有料閲覧
- Abstract 文献概要
- 1ページ目 Look Inside
- 参考文献 Reference
はじめに Stanford B型大動脈解離に対する胸部ステントグラフト内挿術(thoracic endovascular aortic repair:TEVAR)はその適応が拡大されつつあり,手術例も増加傾向にある1).しかし,TEVAR後の逆行性Stanford A型大動脈解離(retrograde Stanford type A dissection:RTAD)は重篤な合併症である.われわれはStanford B型大動脈解離に対するTEVAR後に発生したRTADに対して心尖部送血による体外循環で緊急手術を施行し,合併症なく救命できた1例を経験したので報告する.
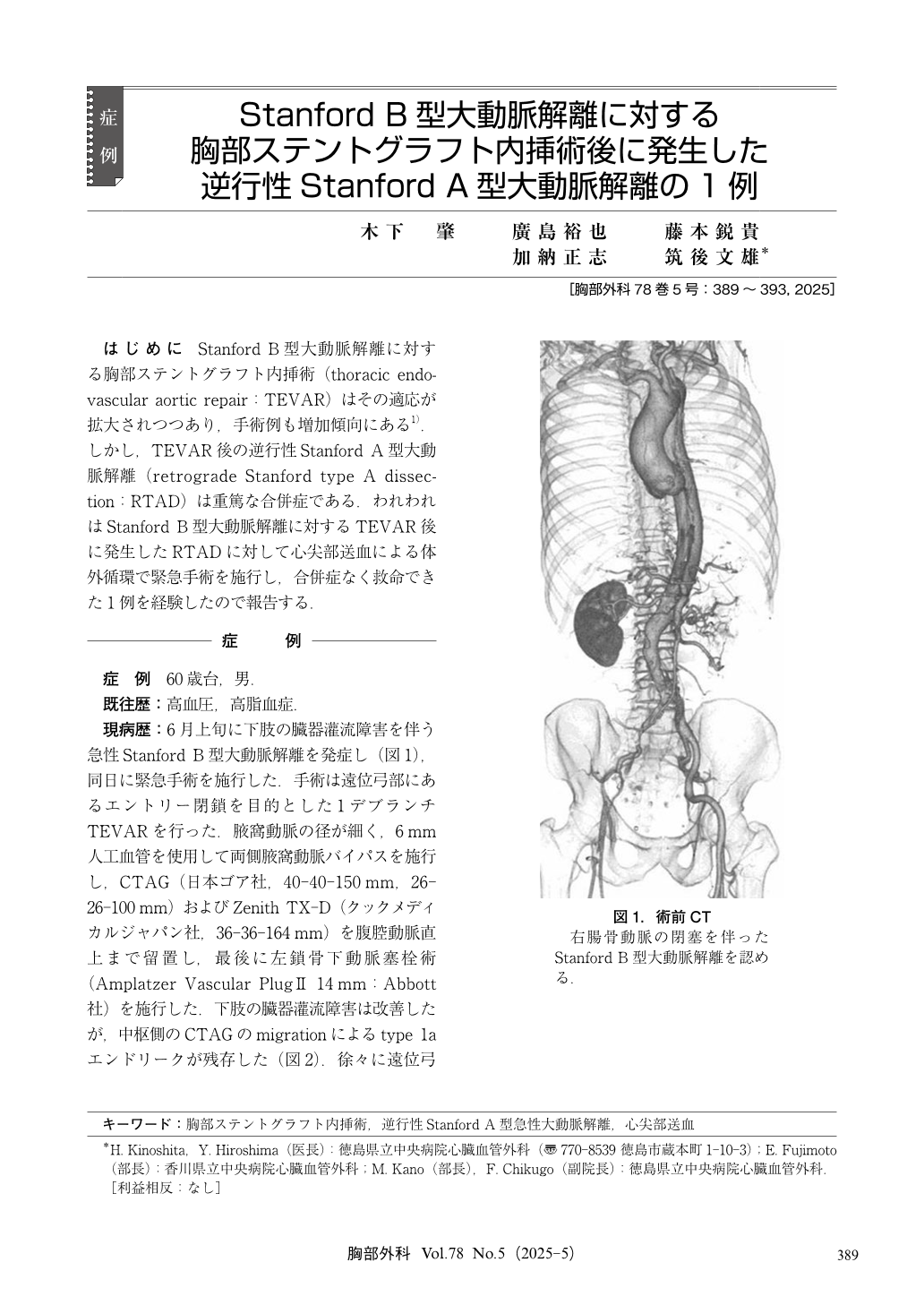
A male patient in his 60s developed acute Stanford type B aortic dissection with malperfusion of the lower limbs in early June. Emergency surgery was performed. The surgery aimed to close the entry in the distal arch and involved a debranched thoracic endovascular aortic repair (TEVAR). Postoperatively, malperfusion improved, but a type 1a endoleak persisted, and the distal arch aneurysm enlarged. Therefore, an additional TEVAR was performed in early October. Compared to the previous procedure, this TEVAR was placed just after the brachiocephalic artery in the central side. One week after surgery, the patient experienced severe chest pain in the early morning, prompting an emergency computed tomography (CT) scan. The diagnosis was retrograde type A aortic dissection (RTAD), and urgent surgery was planned. While considering blood supply options, the possibility of using blood from the previously debranched artificial vessel was evaluated. However, due to concerns about the narrow diameter of the artificial vessel and ensuring sufficient full flow, blood supply was performed from the cardiac apex. The entry of the dissection was located at the level of the brachiocephalic artery on the lesser curvature side, and an ascending arch aortic replacement was performed. The patient was extubated the day after surgery, and the postoperative course was favorable. The choice of blood supply for RTAD remained a challenge. Despite the risk of malperfusion with retrograde femoral artery blood supply, the surgeon chose the familiar cardiac apex approach, ultimately saving the patient’s life.
© Nankodo Co., Ltd., 2025

