Japanese
English
- 有料閲覧
- Abstract 文献概要
- 1ページ目 Look Inside
I.はじめに
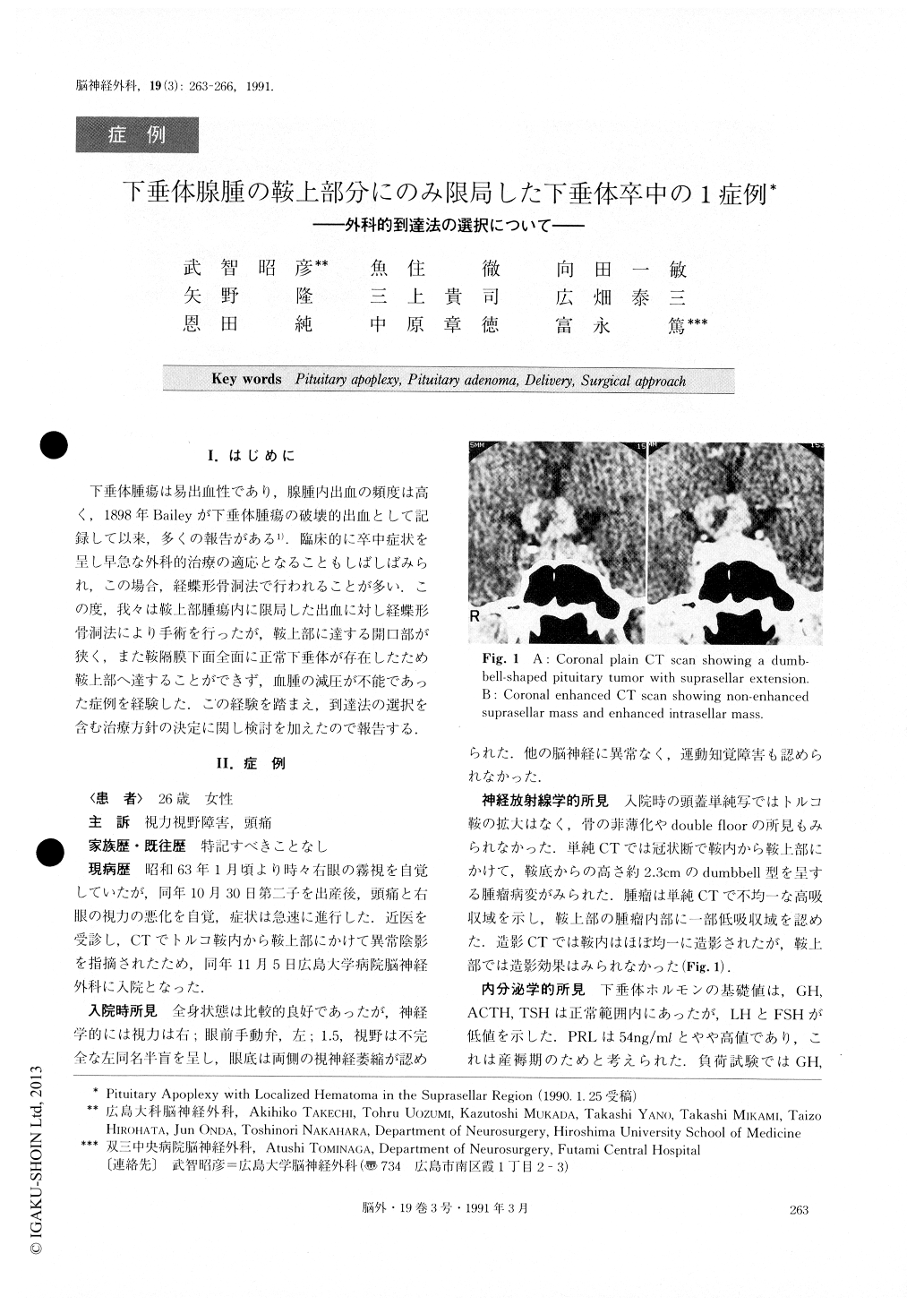
下垂体腫瘍は易出血性であり,腺腫内出血の頻度は高く,1898年Baileyが下垂体腫瘍の破壊的出血として記録して以来,多くの報告がある1).臨床的に卒中症状を呈し早急な外科的治療の適応となることもしばしばみられ,この場合,経蝶形骨洞法で行われることが多い.この度,我々は鞍上部腫瘍内に限局した出血に対し経蝶形骨洞法により手術を行ったが,鞍上部に達する開口部が狭く,また鞍隔膜下面全面に正常下垂体が存在したため鞍上部へ達することができず,血腫の減圧が不能であった症例を経験した.この経験を踏まえ,到達法の選択を含む治療方針の決定に関し検討を加えたので報告する.
Abstract
The authors report a case of a patient with a pitui-tary tumor, in which pituitary apoplexy occurred only in the suprasellar part of the tumor.
A 26-year-old woman suffered from abrupt worsen-ing of vision and headache. A CT scan showed a dumb-bell-shaped tumor extending to the suprasellar region, in which an irregularly shaped low density area sug-gesting a liquidized hematoma was seen. The rapid worsening of her symptoms was highly indicative of pituitary apoplexy. The first operation was performed through the transsphenoidal route. There was no evi-dence of intratumoral hematoma in the intrasellar tumor, wihch could be removed successfully. However, the suprasellar mass could not be reached because of the hardness of the diaphragma sellae and the presence of a normal pituitary gland. MRI and CT cisternogra-phy after this first operation showed a narrow opening of the diaphragma sellae. The second operation using right frontotemporal craniotomy disclosed a suprasellar mass, wihich consisted of an old hematoma and a necrotic tumor. The tumor was sub-totally removed. The patient's visual acuity improved after the second operation. Although transsphenoidal surgery is the treatment of choice in patients with pituitary apoplexy, the selection of the surgical route should be made only after careful neuroradiological evaluation with regard to the extrasellar extension of the tumor.
Copyright © 1991, Igaku-Shoin Ltd. All rights reserved.

