Japanese
English
- 有料閲覧
- Abstract 文献概要
- 1ページ目 Look Inside
緒言
頭部外傷の脳波に関して,従来多数の報告があるが,その多くは軽症から重症までの頭部外傷を一括して取扱つたもので,病型別に脳波を観察した報告は意外に少ない。
われわれは,すでに,本誌に「外傷性頭蓋内血腫術後の脳波26)」について発表している。さきに,外傷性頭蓋内血腫症例のみを取扱つた理由は,このような症例では開頭術が実施されており,脳の損傷部位と病変が手術時に確かめられているので,術後の脳波を検討する上に有利で,血腫症例における術後の臨床脳波的推移はどうか,外傷性てんかんとの相関性はどうかなどを,他の頭部外傷から切り離して検討しようと意図したためである。
In 1948, C. Araki classified head injury cases into4 types, namely, the simple type (1st type), thecerebral concussion type (2nd type), the cerebralcontusion type (3rd type) and the intracranialhemorrhage type (4th type).
This classification has been widely used in Japanfor diagnosis and estimation of severity of headinjury cases.
For past 4 years, many cases of head injury weretreated at the Neurosurgical Department of OsakaRed Cross Hospital. Previously we made a reportof "Postoperative Electroencephalographic Studiesof Traumatic Intracranial Hematoma Cases."
In this paper, 26 cases of the cerebral contusiontype and 28 cases of the intracranial hemorrhagetype, in which early death cases and traumatic in-tracranial hematoma cases were excluded, wereexamined with 57 and 43 successive EEG records,respectively.
The period of EEG recording extended from thefirst day to 3 years after the head injury in the3rd type, and from first day to 3 years and 4months in the 4th type.
A) Summary of clinical findings was as follows.
In the 3rd type, average duration of loss of con-sciousness was 22 days. Of 26 cases, conjugatedeviation of eye balls was found in 4, decerebraterigidity in 4, motor palsy in 12, motor aphasia in1, early epilepsy in 6 (generalized 4, focal 2) andskull fracture in 11. Prognosis of the 3rd type wasgrave in general.
In the 4th type, initial loss of consciousness wasdetected in 13 of 28 cases. Duration of lucid in-terval was less than one hour in 18 cases, it wasbetween one hour and 24 hours in 8 cases, and itwas more than 24 hours in 2 cases. Of 28 cases,early epilepsy was observed in 25 (generalized 20,focal 4 Jacksonian 1), and skull fracture in 10.Prognosis of this 4th type was very good.
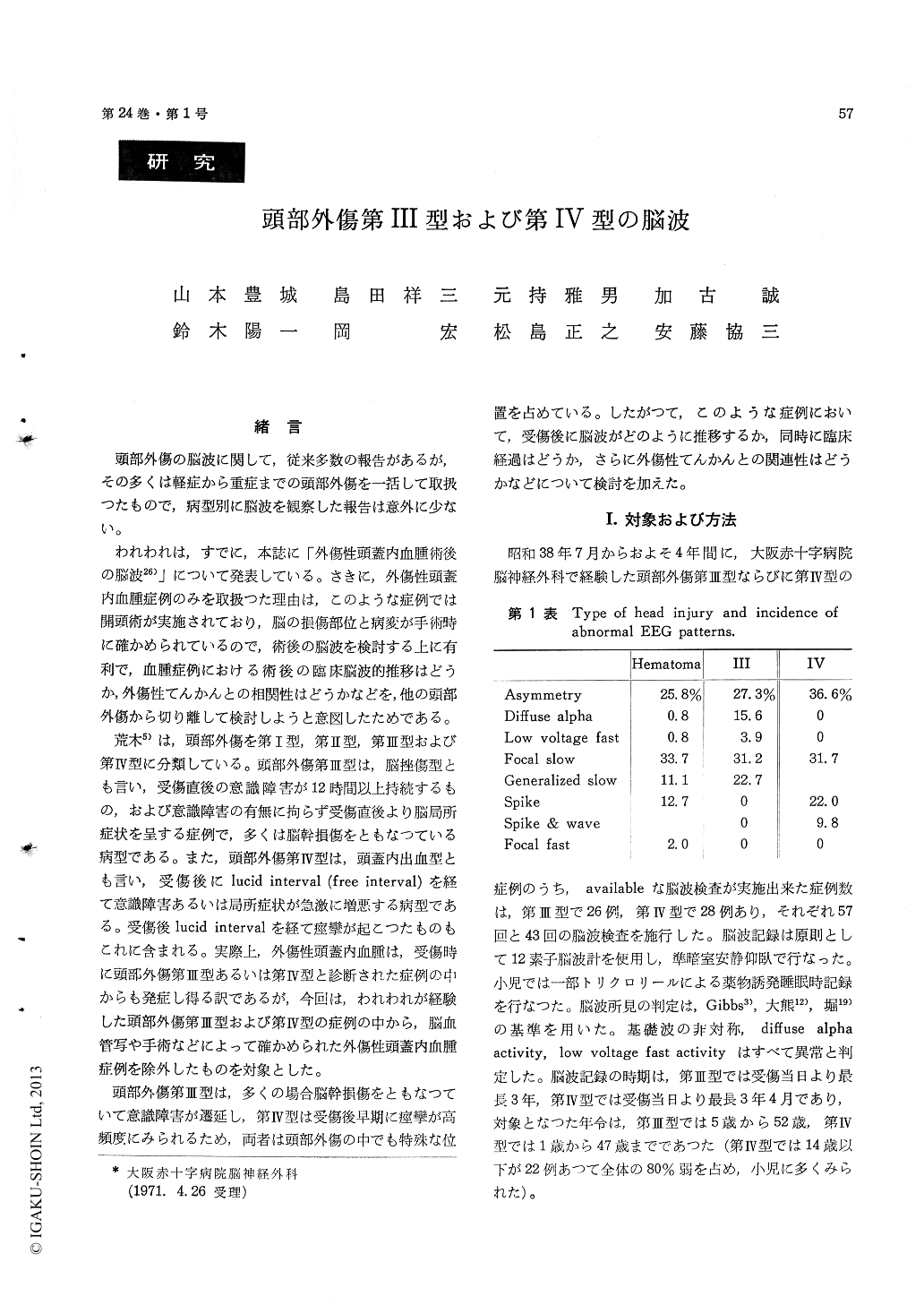
B) The classification of abnormal EEG patternsand their incidences were as follows.
In the 3rd type, diffuse alpha activity was seenin 15.6%, low voltage fast activity 3.9%, asym-metry 27.3%, focal slow wave 31.2%, and genera-lized slow wave 22.7%. There was no seizuredischarge at all.
In the 4th type, asymmetry was seen in 36.6%,focal slow wave 31.7%, focal spike 22.0%, andwave complex 9.8%.
C) Characteristic EEG features of the 3rd typewere as follows.
1) EEG abnormality was found in high frequen-cy (82.5%), 2) focal slow wave was main abnormalEEG pattern, 3) no seizure discharge was detectedat all, and 4) EEG abnormality was apt to persistfor a long time after head injury.
D) Characteristic EEG features of the 4th typewere as follows.
1) EEG abnormality was also found in highfrequency (55.8%), 2) seizure discharge was morefrequently seen in the 4th type than in other headinjury types, and 3) there were two ways in nor-malizing EEG process, namely the one in whichEEG changes were getting better in short span oftime, and the other in which EEG changes showedno or little progress toward recovery for a longtime.
E) Posttraumatic epilepsy occurred in no casefrom the 3rd type and in 2 cases from the 4th type.Although it has been conceivable that cerebral con-tusion may lead to focal lesion of meningocerebralcicatrix and/or cerebral cicatrix in convalescentperiod, which may form epileptogenic focus, it isinteresting fact that no posttraumatic epilepsy hasdeveloped from the patients of the cerebral con-tusion type, which seems to be rather severe headinjury.
Copyright © 1972, Igaku-Shoin Ltd. All rights reserved.

