Japanese
English
- 有料閲覧
- Abstract 文献概要
- 1ページ目 Look Inside
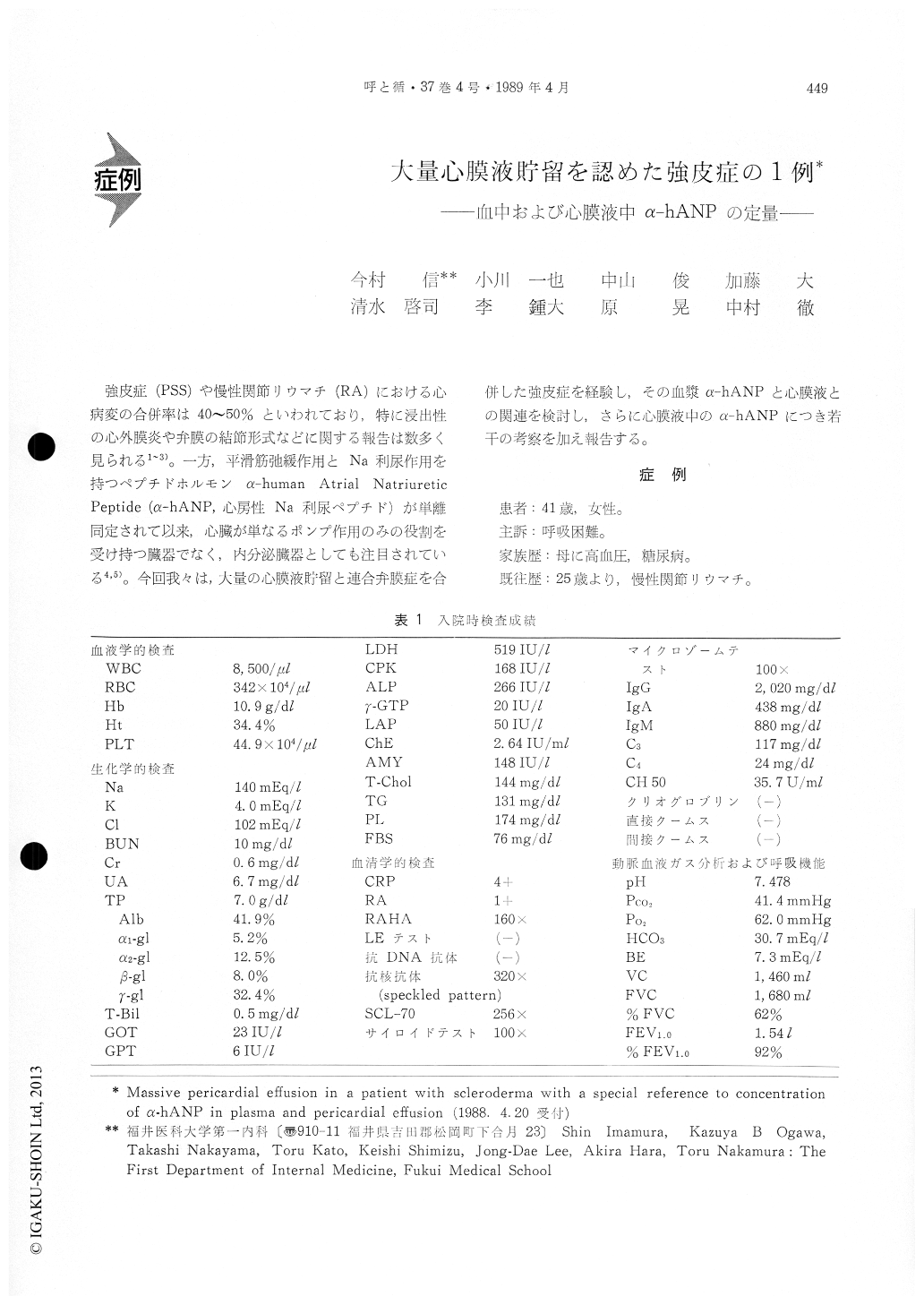
強皮症(PSS)や慢性関節リウマチ(RA)における心病変の合併率は40〜50%といわれており,特に浸出性の心外膜炎や弁膜の結節形式などに関する報告は数多く見られる1〜3)。一方,平滑筋弛緩作用とNa利尿作用を持つペブチドホルモンα-human Atrial NatriureticPeptide (α-hANP,心房性Na利尿ペプチド)が単離同定されて以来,心臓が単なるポンプ作用のみの役割を受け持つ臓器でなく,内分泌臓器としても注目されている4,5)。今回我々は,大量の心膜液貯留と連合弁膜症を合併した強皮症を経験し,その血漿α-hANPと心膜液との関連を検討し,さらに心膜液中のα-hANPにつき若干の考察を加え報告する。
A 41-year-old woman was admitted to our hospital because of scleroderma and combined valvular dis-ease (mitral stenosis, aortic regurgitation, tricuspid regurgitation) associated with massive pericardial effusion. Plasma atrial natriuretic peptide (α-hANP) level was 130 pg/ml on admission, and increased temporarily with a decrease of pericardial effusion, without significant of changes of pulmonary capillary wedge pressure, pulmonary arterial pressure, right ventricular pressure nor right atrial pressure. These findings suggest that one of the mechanisms of a-hANP secretion, a stretch receptor mechanism, is interfered by the massive pericardial effusion. There was no relationship between atrial pressures and plasma α-hANP levels in this case. α-hANP con-centration in pericardial effusion (486 pg/ml) was four to five folds higher than the plasma a-hANP levels.
Copyright © 1989, Igaku-Shoin Ltd. All rights reserved.

