Japanese
English
- 有料閲覧
- Abstract 文献概要
- 1ページ目 Look Inside
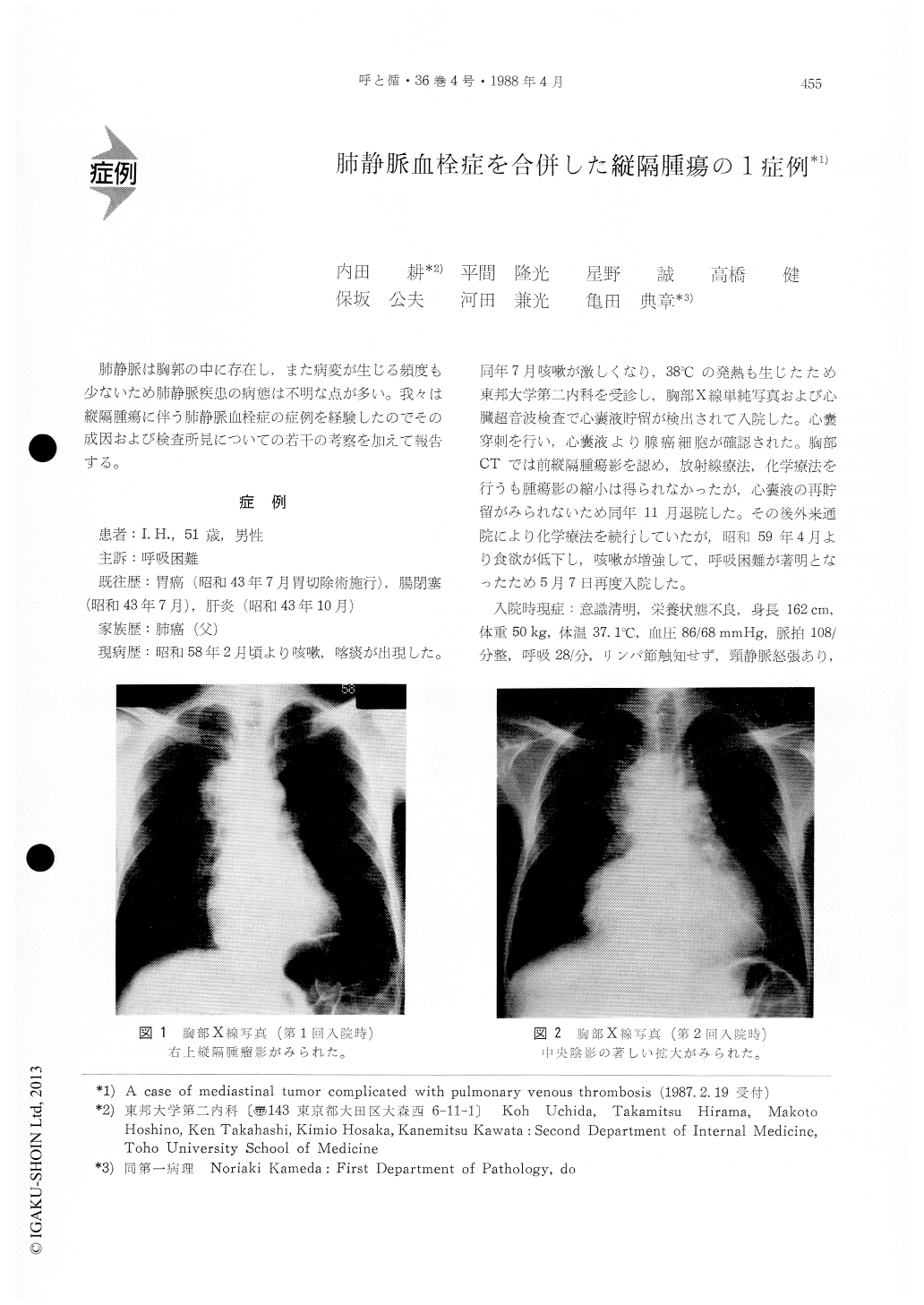
肺静脈は胸郭の中に存在し,また病変が生じる頻度も少ないため肺静脈疾患の病態は不明な点が多い。我々は縦隔腫瘍に伴う肺静脈血栓症の症例を経験したのでその成因および検査所見についての若干の考察を加えて報告する。
A 51-year-old man was admitted in July, 1983 be-cause of cough, sputum and fever. Roentgenogra-phic and echocardiographic findings suggested pres-ence of a mediastinal tumor and pericardial effusion. Neoplastic cells (adenocarcinoma) were detected inthe pericardial effusion. Radiation therapy and che-motherapy were administered ; the morbid nest sho-wed no change and he was discharged in November 1983. The patient was readmitted in May, 1984 because of worsening of cough and dyspnea. On physical examination there were evident jugular venous dilatation and cyanosis of the lips. Nume-rous dry rales were heard over both lung fields. Blo-od gas analysis revealed remarkable hypoxemia (PaO240.4 Torr) with hypocapnia (PaCO2 27.6 Torr) despite oxygen administration (FiO2 0.5). An electrocardiog-ram showed right axis deviation. A chest roentge-nogram showed marked enlargement of the cardiac and mediastinal shadows without findings of pulmo-nary edema. A gamma camera lung scan recorded during inhalation of 81mKripton gas and after intra-venous injection of 10 mCi of 99mTc-macroaggregate demonstrated a decreased ventilation in the left lung with normal ventilation image in the right lung and numerous small wedgeshaped perfusion defects in both lung fields. After admission, hypoxemia per-sisted even with 100% oxygen inhalation. Numerous moist rales were heard in the bases of both lungs for the-first-time on the second hospital day. The patientbecame unresponsive and died on the third hospital day. Post-mortem examination disclosed a large tu-mor mass (15×10×10cm) which occupied the right anterior portion to the heart, which distorted the heart and compressed pulmonary vessels. The his-tology of the tumor was poorly differentiated adeno-carcinoma. There were multiple thrombi in the pe-ripheral and central pulmonary veins of both lungs. There was no gross nor microscopic evidence of pul-monary or systemic arterial emboli or infarctions.
Initial symptomes in this case were due to peri-cardial effusion which was induced by invasion of mediastinal tumor to the pericardium. Ten months later, he died of multiple pulmonary venous throm-bosis. A compression of the pulmonary veins and heart by the tumor mass was considered to be the main factor for the genesis of thrombosis rather than coagulation abnormalities. The origin of the tumor was not clarified. In this case it was made clear that the occlusion of pulmonary veins without pulmonary arterial thrombosis caused the severe hypoxemia and the multiple filling defects noted on perfusion scintigram.
Copyright © 1988, Igaku-Shoin Ltd. All rights reserved.

