Japanese
English
- 有料閲覧
- Abstract 文献概要
- 1ページ目 Look Inside
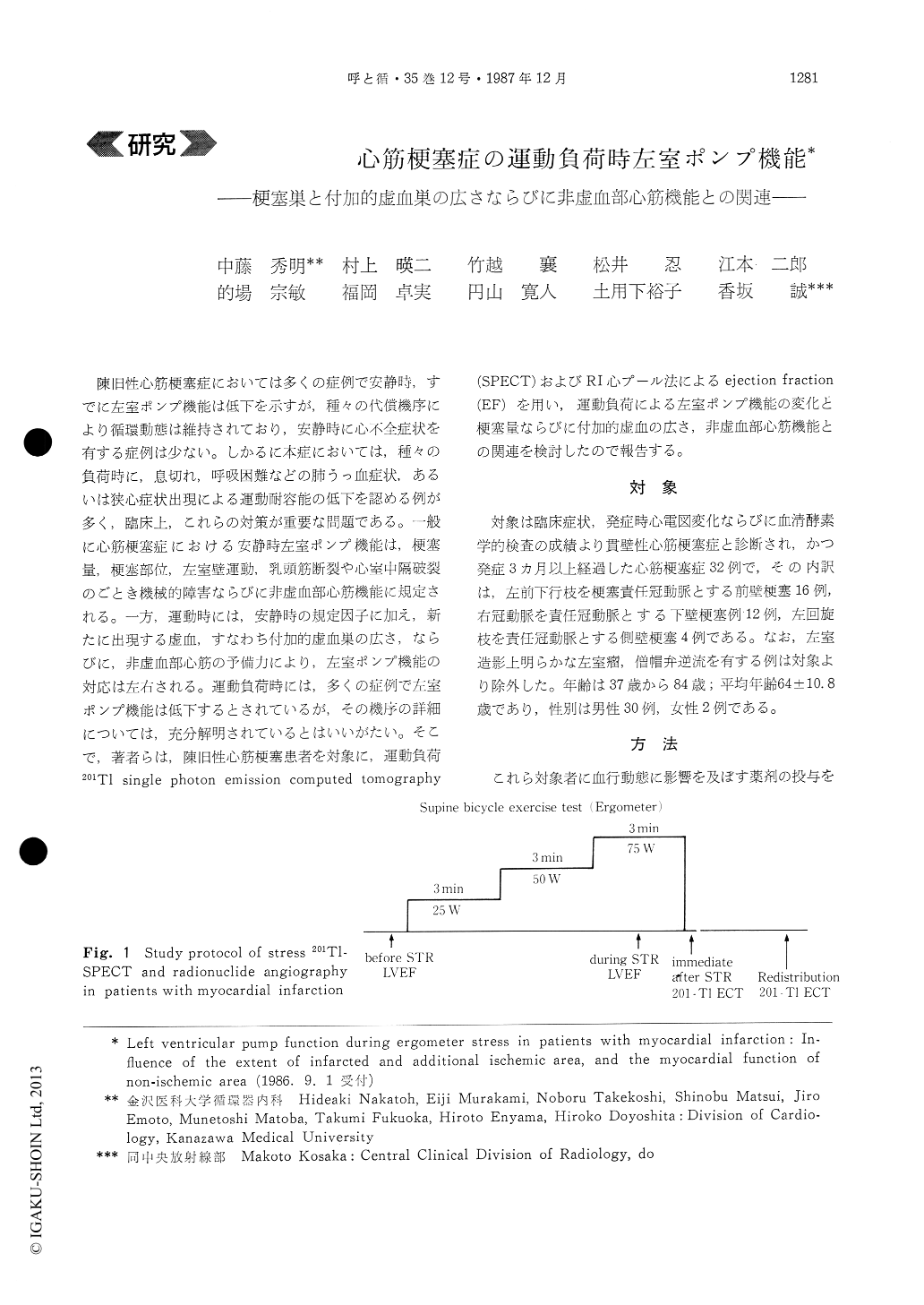
陳旧性心筋梗塞症においては多くの症例で安静時,すでに左室ポンプ機能は低下を示すが,種々の代償機序により循環動態は維持されており,安静時に心不全症状を有する症例は少ない。しかるに本症においては,種々の負荷時に,息切れ,呼吸困難などの肺うっ血症状,あるいは狭心症状出現による運動耐容能の低下を認める例が多く,臨床上,これらの対策が重要な問題である。一般に心筋梗塞症における安静時左室ポンプ機能は,梗塞量,梗塞部位,左室壁運動,乳頭筋断裂や心室中隔破裂のごとき機械的障害ならびに非虚血部心筋機能に規定される。一方,運動時には,安静時の規定因子に加え,新たに出現する虚血,すなわち付加的虚血巣の広さ,ならびに,非虚血部心筋の予備力により,左室ポンプ機能の対応は左右される。運動負荷時には,多くの症例で左室ポンプ機能は低下するとされているが,その機序の詳細については,充分解明されているとはいいがたい。そこで,著者らは,陳旧性心筋梗塞患者を対象に,運動負荷201T1 single photon emission computed tomography(SPECT)およびRI心プール法によるejection fraction(EF)を用い,運動負荷による左室ポンプ機能の変化と梗塞量ならびに付加的虚血の広さ,非虚血部心筋機能との関連を検討したので報告する。
This study examines the relation between the extent of myocardial necrosis-ischemia and the left ventricular (LV) ejection fraction (EF) response to ergometer stress in patients with myocardial infarc-tion (MI). We studied 32 patients with MI aged 37 to 84 years by radionuclide ventriculography (at rest and during stress) and by stress 201Tl single photon emission computed tomography (SPECT).
During stress, mean blood pressure (MBP) and heart rate (HR) were increased significantly (MBP : 91±13.4→ 109±17.6 mmHg p<0.005, HR : 67±9.0→106±17.6 bpm/min p<0.001). EF was decreased from 37±12.0 to 34±10.8% and 201 Tl defect was increased from 15±11.8 to 20±12.3%, both signifi-cantly (EF p<0.05, 201 Tl defect p<0. 05). During stress, 20 of 32 patients showed an increased 201 T1 defect and a decreased EF, 7 an increased 201 Tl defect and EF, 5 a decreased 201 T1 defect and EF. The change in 201T1 defect (Δd201 T1 defect) during stress did not correlate with that in EF (ΔIEF).
Both before and during stress, there were signi-ficant regressions between 201T1 defect (%) and EF (%). The regression lines were y=-0.730x+48.46before stress (p<0.001) and y=-0.632x+ 47. 19 during stress (p<0.001), where y is EF and x is 201T1 defect. There was no singnificant difference between these two regression lines.
These data suggest that LV pump function during stress in patients with MI could be regulated mainly by the extent of necrotic and ischemic area, and partially by the regional myocardial function of non-ischemic area.
Copyright © 1987, Igaku-Shoin Ltd. All rights reserved.

