Japanese
English
- 有料閲覧
- Abstract 文献概要
- 1ページ目 Look Inside
Sjögren症候群(SjS)は,臨床的に口内乾燥症・乾燥性角結膜を主徴とする外分泌腺の慢性炎症性疾患である。慢性関節リウマチ(RA)や全身性エリテマトーデス(SLE)などの結合織疾患(CTD)を伴うものがあり,病因に自己免疫機序が考えられている。外分泌腺の機能異常に加え,発熱などの全身症状,さらに多発性関節炎・Raynaud現象・皮疹,肺・肝・腎病変など多臓器障害症状が報告されている1〜5)。肺病変として気道の乾燥症とそれに続発する感染症のほかに、間質性肺炎,肺線維症が知られているが,その頻度は数%〜10数%と低率である6,7)。さらに肺高血圧症(PH)はきわめて稀で,本邦では河野らの一例報告8)があるにすぎない。
我々は,顕著なRaynaud現象を伴いPHを呈したSjSの一例を経験した。SjSの病態およびPHの成因を考えるうえで重要な症例と思われるので報告する。
A 31-year old woman with Sjögren syndrome (SjS) and pulmonary hypertension (PH) was report-ed. She was well until 8 years prior to admission(PTA), when she first noticed dryness of eyes and mouth. Nine months PTA, she started to have easy fatigability and exertional dyspnea. Subsequently she noticed to have Raynaud's phenomenon of her fingers. Two months PTA, a physician told her that she had cardiomegaly and a positive rheumatoid factor. She was admitted to our hospital for further evaluation.
On physical exam. her temperature was 37.4C degree, pulse rate was 100 regular. Blood pressure was 84/68. The patient was without distress, though she appeared to be somewhat pale. Raynaud's phenomenon was observed on her fingers. There was no cyanosis, no clubbing. On cardiac exam. there was a right ventricular (RV) heave with accentuated second pulmonic sound. Right sided S4 was audible. There was no murmur, no rub. Lungs were clear. Carotid and peripheral pulses were normal. There was no jugular venous distension, hepatomegaly nor edema.
Laboratory values were as follows: hematocrit, 32.6; WBC, 2900; platelet, 90000; ESR, 67/ hour; protein, 7.7g/di; gamma globulin, 3.3g/di; IgG, LgA, LgM, 4605, 310, 190mg/dI respectively; rheumatoid factor, positive; RAHA titer, 1: 1280; ANA, positive; titer, 1: 512 with specled pattern; anti-RNP, anti-SSA, anti-SSB, positive; anti-DNA (binding assey), 12% (normal, less than 20%); serum complements, C3 25mg/dl; cryoglobulin, positive with IgG-IgM component.
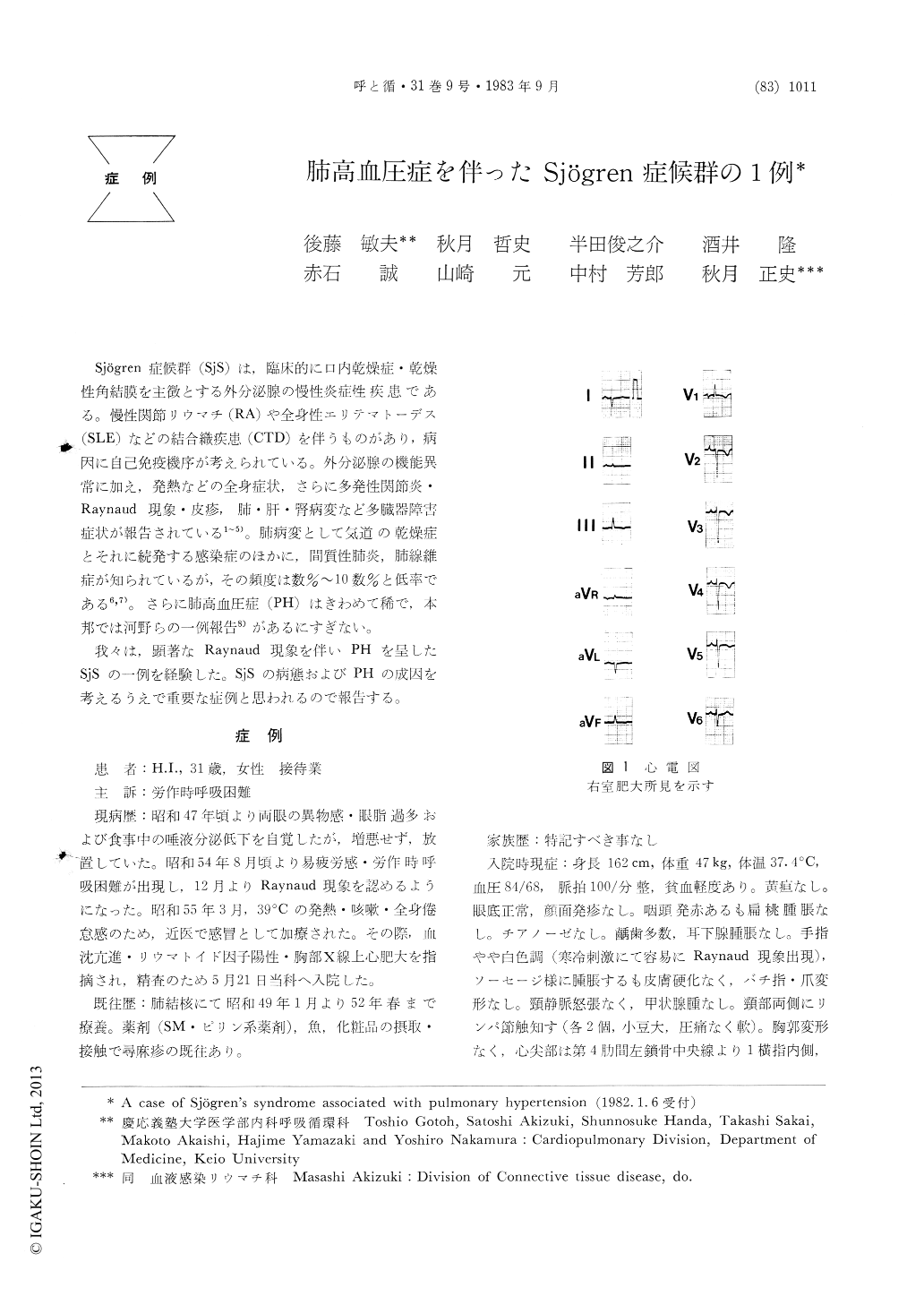
A Schirmer test was positive. A sialogrm showed a typical branchless tree pattern. A slivary scintigram revealed markedly reduced uptake of the parotid glands. A labial biopsy showed a chronic inflammatory change. An ECG showed RV hypertrophy.A chest X-ray revealed RV enlargement and the prominent central pulmonary arteries. Pulmonary function studies demonstrated that %VC was 74, FEV 1.0% was 82. DLco was 5.0 ml/mimtor. Arterial blood gas showed Po2 of 61mmHg, Pco2 of 24mmHg and PH of 7.51. A lung scan demonstrated no segmental perfusion defects. Right heart catheterization revealed PA pressure of 50/28mmHg with mean of 36mmHg. Mean pulmonary capillary wedge pressure was 5 mmHg. No intracardiac shunt was seen.
Prednisolone of 20mg (po) was given with remis-sion of fatigue and subfever. The patient felt slight improvement of dry eyes and mouth.
SjS associated with PH was a rare combination. This is the second case reported in Japan. The PH in this case was assumed to be mainly caused by imvolvement of pulmonary arteries. Normal lung fields in chest x-ray, slight restrictive ventilatory impairement and markedly decreased DLco were observed. We suspected that the pulmonary arterial imvolvement was closely related to Raynaud's phenomenon and/or marked immmunological abnormalities of SjS including immmune com-plexes.
Copyright © 1983, Igaku-Shoin Ltd. All rights reserved.

