Japanese
English
- 有料閲覧
- Abstract 文献概要
- 1ページ目 Look Inside
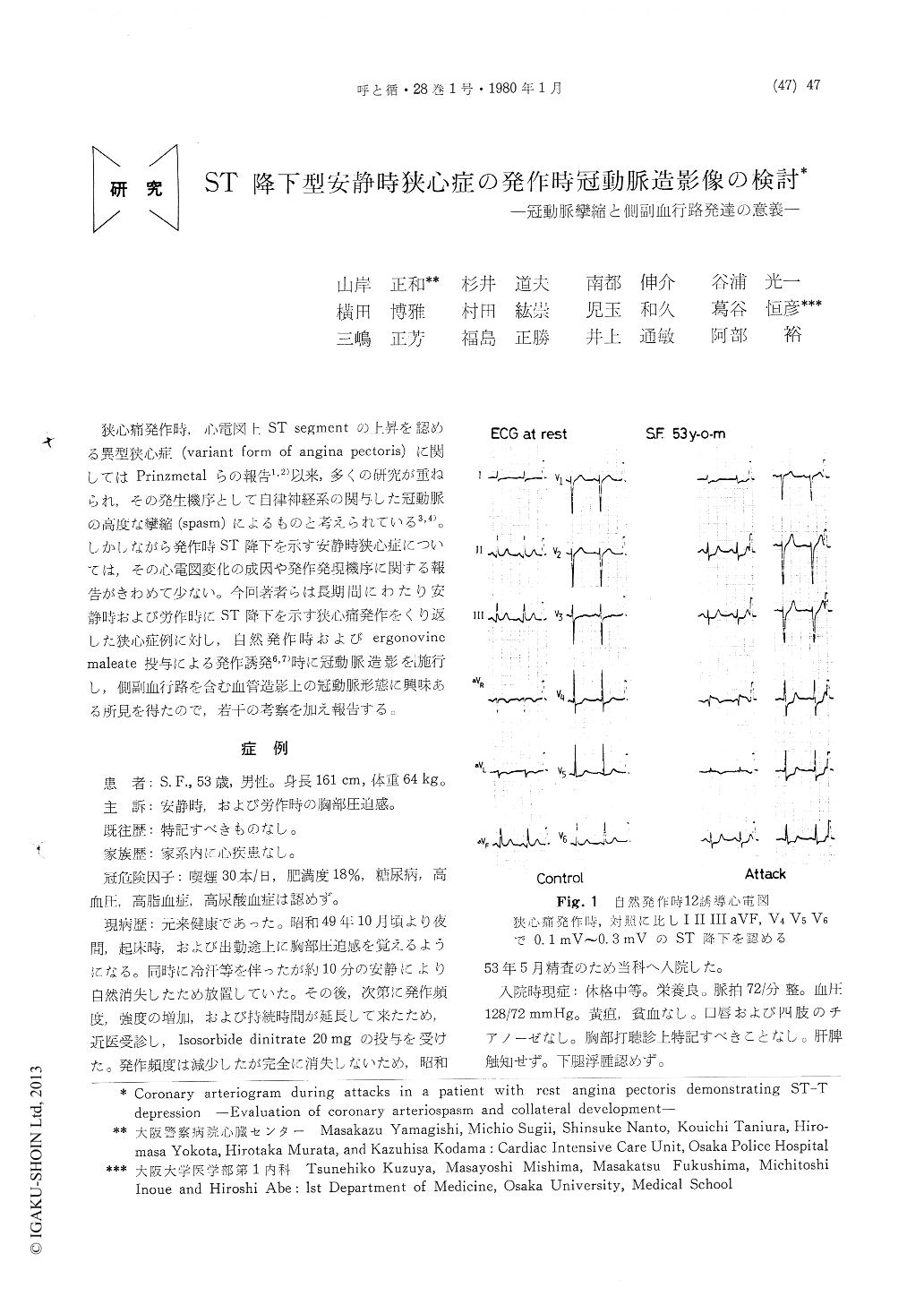
狭心痛発作時,心電図上ST segmentの上昇を認める異型狭心症(variant form of angina pectoris)に関してはPrinzmetalらの報告1,2)以来,多くの研究が重ねられ,その発生機序として自律神経系の関与した冠動脈の高度な攣縮(spasm)によるものと考えられている3,4)。しかしながら発作時ST降下を示す安静時狭心症については,その心電図変化の成因や発作発現機序に関する報告がきわめて少ない。今回著者らは長期間にわたり安静時および労作時にST降下を示す狭心痛発作をくり返した狭心症例に対し,自然発作時およびergonovinemaleate投与による発作誘発6,7)時に冠動脈造影を施行し,側副血行路を含む血管造影上の冠動脈形態に興味ある所見を得たので,若干の考察を加え報告する。
A 53 year old man began to complain of an-terior chest oppression at rest and at exertion in Oct. 1974. The symptom was relieved within 10 min. with nitroglycerin or by rest. However, his complaint had gradually increased in frequ-ency and he was admitted to our clinic forexamination in detail in May 1978. Physical and laboratory findings were almost normal. He didn't have the coronary risk factors except for smoking and mild obesity. Longterm electro-cardiographic monitoring (by the Holter Avionics System) showed severe ST-T segment depression several times over night. The exercise stress test by the bicycle ergometer failed to provoke an angina at the first trial but a typical anginal attack at the second trial with severe ST-T seg-ment depression in leads II, III, aVF, and V4 to V6. Coronary arteriography was performed on a morning in Feb. 1979. When a spontaneous anginal attack attended by ST-T segment de-pression occured, the left coronary arteriogram showed subtotal occlusion at the main trunk and the proximal portion of the LAD. The anginal attack was promptly relieved with nitroglycerin, and the left coronary arteriogram then taken showed almost normal visualization, and no organic stenosis existed. When an anginal attack was provoked by ergonovine maleate, the electro-cardiogram showed the same ST-T segment de-pression that as at spontaneous attack, and the left coronary arteriogram showed almost total occlusion at the proximal portion of the LAD. The right coronary artery was normal on the control arteriogram, but significant collaterals to the LAD appeared during an anginal attack at-tended by the same ST-T segment depression as before, and it disappeared after nitroglycerin medication. At last, multiple projection was performed and we confirmed no organic stenosis anywhere. Thus, we diagnosed this case as ST-T segment depressive vasospastic angina pectoris without organic stenosis.
Transient collateral visualization during vaso-spasm had already been observed by several workers, but no such significant collateral de-velopement with normal coronary has been de-scribed. Generally an organic stensis over 50 percents is necessary for the development of the collaterals, but in this case a severe vasospasm played the same part as an organic stenosis and the collaterals developed which was influential on the ST-T segment shift of the electrocardio-gram. As a conclusion, we consider that the vasospastic angina attended by ST-T segment depression, in which the coronary arteriogram showed no organic stenosis after disappearance of spasm, could have significant collaterals: therefore, it is important to perform angiography on the opposite side of spastic artery in such a case.
Copyright © 1980, Igaku-Shoin Ltd. All rights reserved.

